

Associations between Aircraft Noise Exposure and Self-Reported Sleep Duration and Quality in the United States-Based Prospective Nurses' Health Study Cohort
- PMID: 37058435
- PMCID: PMC10104165
- DOI: 10.1289/EHP10959
Associations between Aircraft Noise Exposure and Self-Reported Sleep Duration and Quality in the United States-Based Prospective Nurses' Health Study Cohort
Abstract
Background: Sleep disruption is linked with chronic disease, and aircraft noise can disrupt sleep. However, there are few investigations of aircraft noise and sleep in large cohorts.
Objectives: We examined associations between aircraft noise and self-reported sleep duration and quality in the Nurses' Health Study, a large prospective cohort.
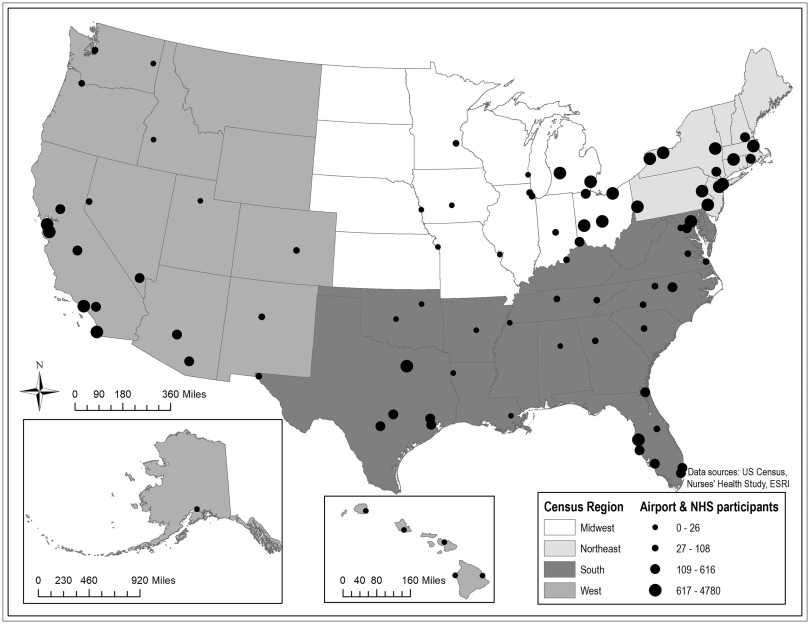
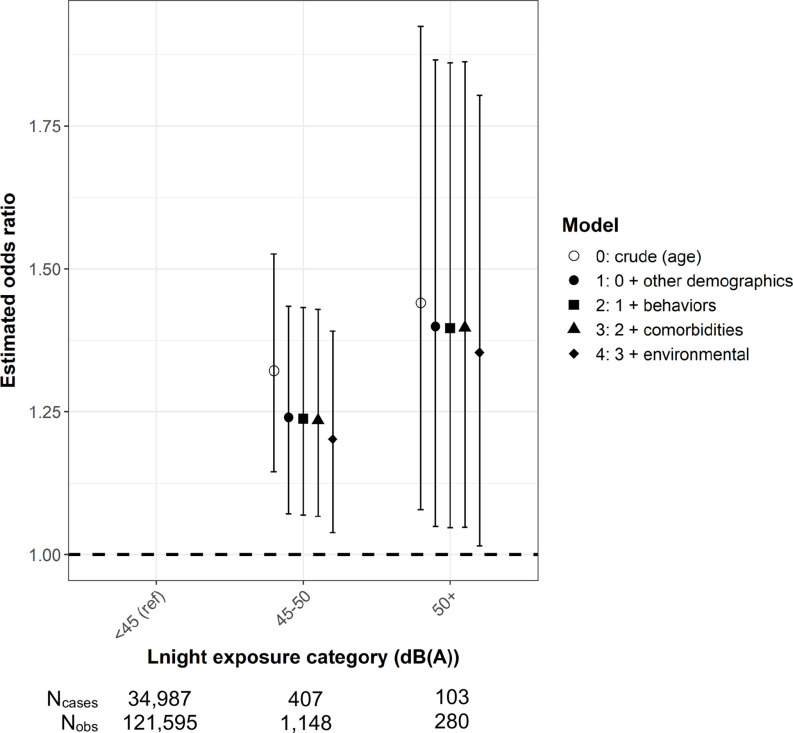
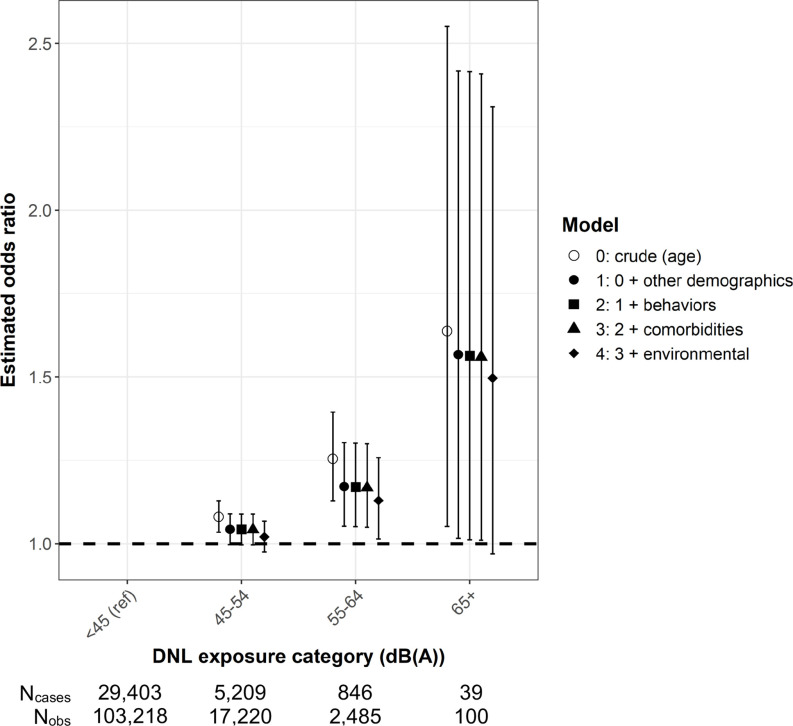
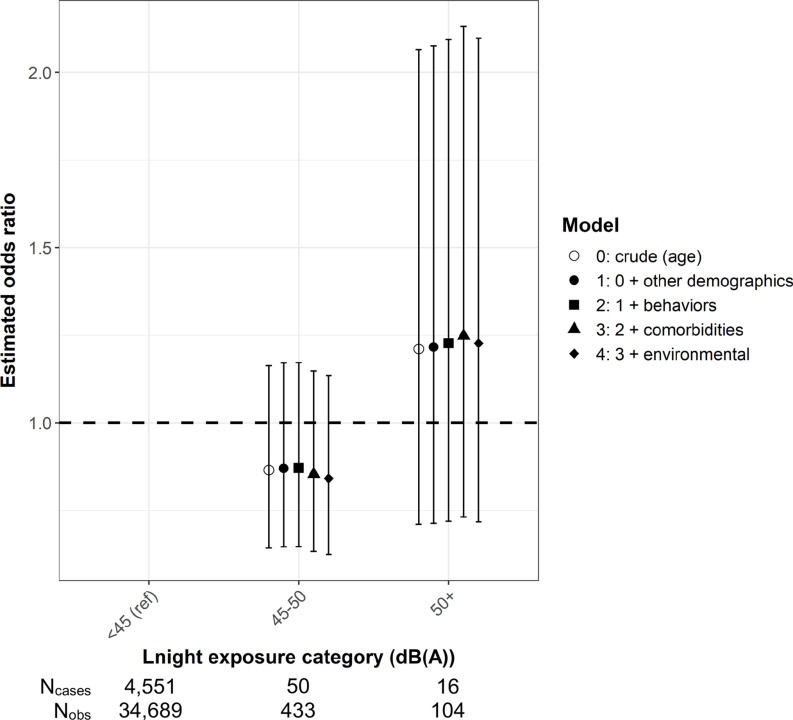
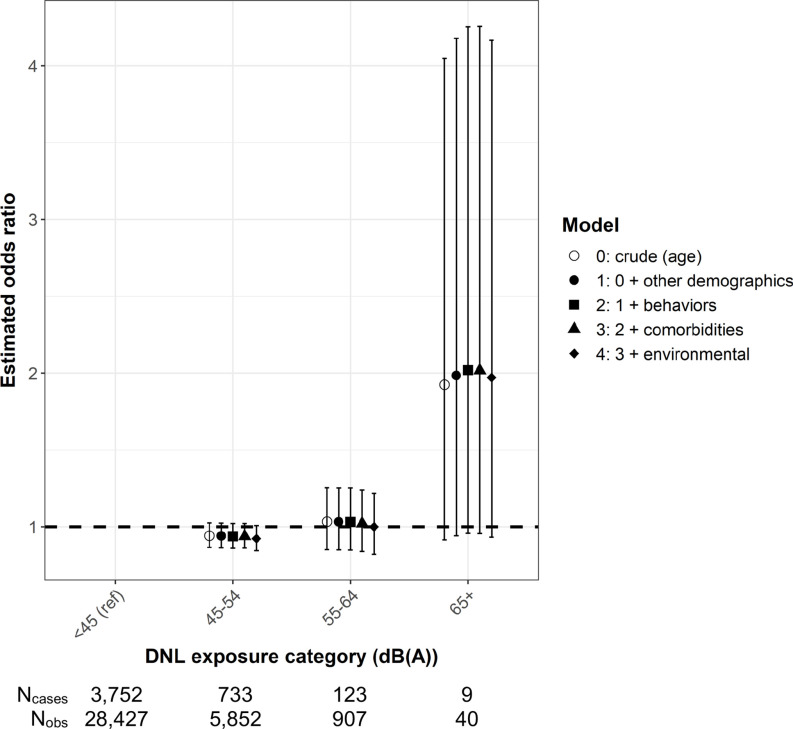
Methods: Aircraft nighttime equivalent sound levels (Lnight) and day-night average sound levels (DNL) were modeled around 90 U.S. airports from 1995 to 2015 in 5-y intervals using the Aviation Environmental Design Tool and linked to geocoded participant residential addresses. Lnight exposure was dichotomized at the lowest modeled level of 45 A-weighted decibels [dB(A)] and at multiple cut points for DNL. Multiple categories of both metrics were compared with dB(A). Self-reported short sleep duration ( h/24-h day) was ascertained in 2000, 2002, 2008, 2012, and 2014, and poor sleep quality (frequent trouble falling/staying asleep) was ascertained in 2000. We analyzed repeated sleep duration measures using generalized estimating equations and sleep quality by conditional logistic regression. We adjusted for participant-level demographics, behaviors, comorbidities, and environmental exposures (greenness and light at night) and examined effect modification.
Results: In 35,226 female nurses averaging 66.1 years of age at baseline, prevalence of short sleep duration and poor sleep quality were 29.6% and 13.1%, respectively. In multivariable models, exposure to Lnight dB(A) was associated with 23% [95% confidence interval (CI): 7%, 40%] greater odds of short sleep duration but was not associated with poor sleep quality (9% lower odds; 95% CI: , 19%). Increasing categories of Lnight and DNL dB(A) suggested an exposure-response relationship for short sleep duration. We observed higher magnitude associations among participants living in the West, near major cargo airports, and near water-adjacent airports and among those reporting no hearing loss.
Discussion: Aircraft noise was associated with short sleep duration in female nurses, modified by individual and airport characteristics. https://doi.org/10.1289/EHP10959.
Figures
Similar articles
-
Aircraft noise exposure and body mass index among female participants in two Nurses' Health Study prospective cohorts living around 90 airports in the United States.Environ Int. 2024 May;187:108660. doi: 10.1016/j.envint.2024.108660. Epub 2024 Apr 15. Environ Int. 2024. PMID: 38677085 Free PMC article.
-
Long-term aircraft noise exposure and risk of hypertension in postmenopausal women.Environ Res. 2023 Feb 1;218:115037. doi: 10.1016/j.envres.2022.115037. Epub 2022 Dec 9. Environ Res. 2023. PMID: 36502895 Free PMC article.
-
Long-term nighttime aircraft noise exposure and risk of hypertension in a prospective cohort of female nurses.Int J Hyg Environ Health. 2025 Jan;263:114457. doi: 10.1016/j.ijheh.2024.114457. Epub 2024 Sep 12. Int J Hyg Environ Health. 2025. PMID: 39270405
-
Aircraft noise-induced awakenings are more reasonably predicted from relative than from absolute sound exposure levels.J Acoust Soc Am. 2013 Nov;134(5):3645-53. doi: 10.1121/1.4823838. J Acoust Soc Am. 2013. PMID: 24180775 Review.
-
Aviation Noise Impacts: State of the Science.Noise Health. 2017 Mar-Apr;19(87):41-50. doi: 10.4103/nah.NAH_104_16. Noise Health. 2017. PMID: 29192612 Free PMC article. Review.
Cited by
-
Endometriosis and uterine fibroids and risk of premature mortality: prospective cohort study.BMJ. 2024 Nov 20;387:e078797. doi: 10.1136/bmj-2023-078797. BMJ. 2024. PMID: 39567014 Free PMC article.
-
Associations between long-term aircraft noise exposure, cardiovascular disease, and mortality in US cohorts of female nurses.Environ Epidemiol. 2023 Jun 21;7(4):e259. doi: 10.1097/EE9.0000000000000259. eCollection 2023 Aug. Environ Epidemiol. 2023. PMID: 37545808 Free PMC article.
-
Aircraft noise exposure and body mass index among female participants in two Nurses' Health Study prospective cohorts living around 90 airports in the United States.Environ Int. 2024 May;187:108660. doi: 10.1016/j.envint.2024.108660. Epub 2024 Apr 15. Environ Int. 2024. PMID: 38677085 Free PMC article.
-
Characterizing temporal trends in populations exposed to aircraft noise around U.S. airports: 1995-2015.J Expo Sci Environ Epidemiol. 2025 Jan;35(1):70-79. doi: 10.1038/s41370-023-00575-5. Epub 2023 Sep 21. J Expo Sci Environ Epidemiol. 2025. PMID: 37735518 Free PMC article.
-
Occupational Exposure to Disinfectants and Risk of Incident Cardiovascular Disease among US Nurses: The Nurses' Health Study II.Environ Health Perspect. 2025 May;133(5):57006. doi: 10.1289/EHP14945. Epub 2025 May 9. Environ Health Perspect. 2025. PMID: 40163383 Free PMC article.
References
-
- Institute of Medicine Committee on Sleep Medicine and Research. 2006. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Colten HR, Altevogt BM, eds. Washington, DC: National Academies Press. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
