

Adjuvant Nivolumab versus Ipilimumab in Resected Stage III/IV Melanoma: 5-Year Efficacy and Biomarker Results from CheckMate 238
- PMID: 37058595
- PMCID: PMC10472092
- DOI: 10.1158/1078-0432.CCR-22-3145
Adjuvant Nivolumab versus Ipilimumab in Resected Stage III/IV Melanoma: 5-Year Efficacy and Biomarker Results from CheckMate 238
Abstract
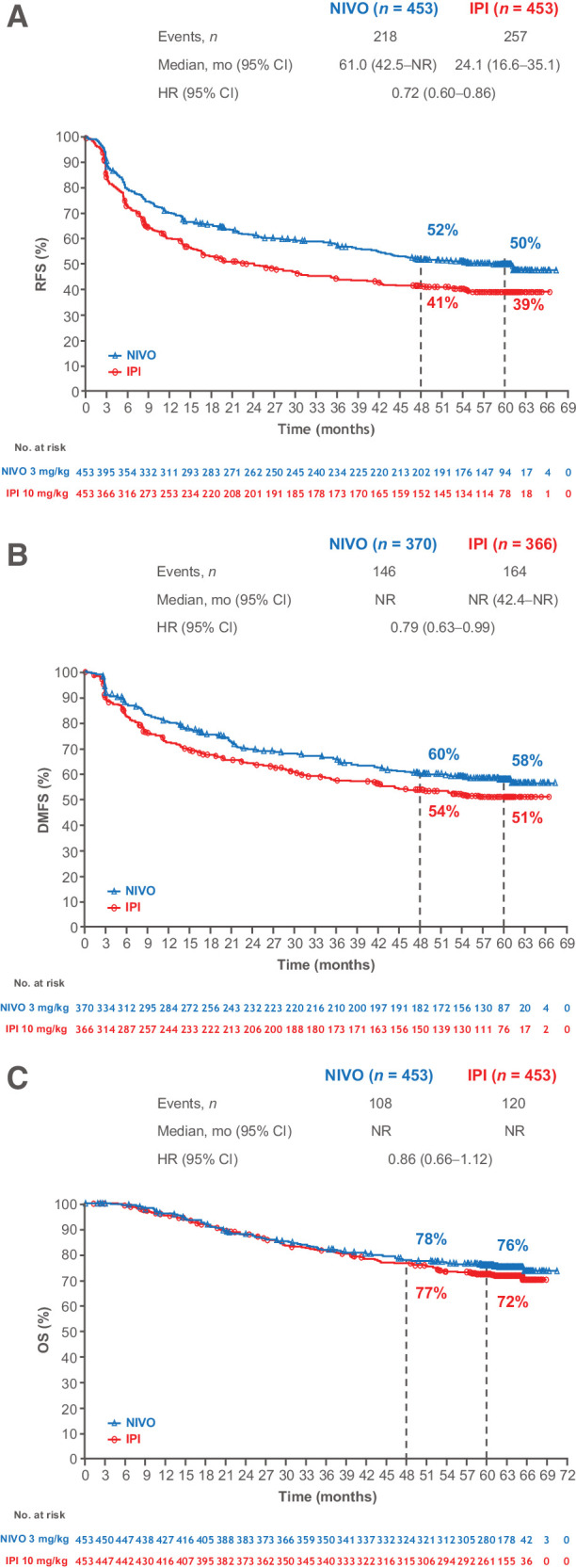
Purpose: In the phase III CheckMate 238 study, adjuvant nivolumab significantly improved recurrence-free survival (RFS) and distant metastasis-free survival versus ipilimumab in patients with resected stage IIIB-C or stage IV melanoma, with benefit sustained at 4 years. We report updated 5-year efficacy and biomarker findings.
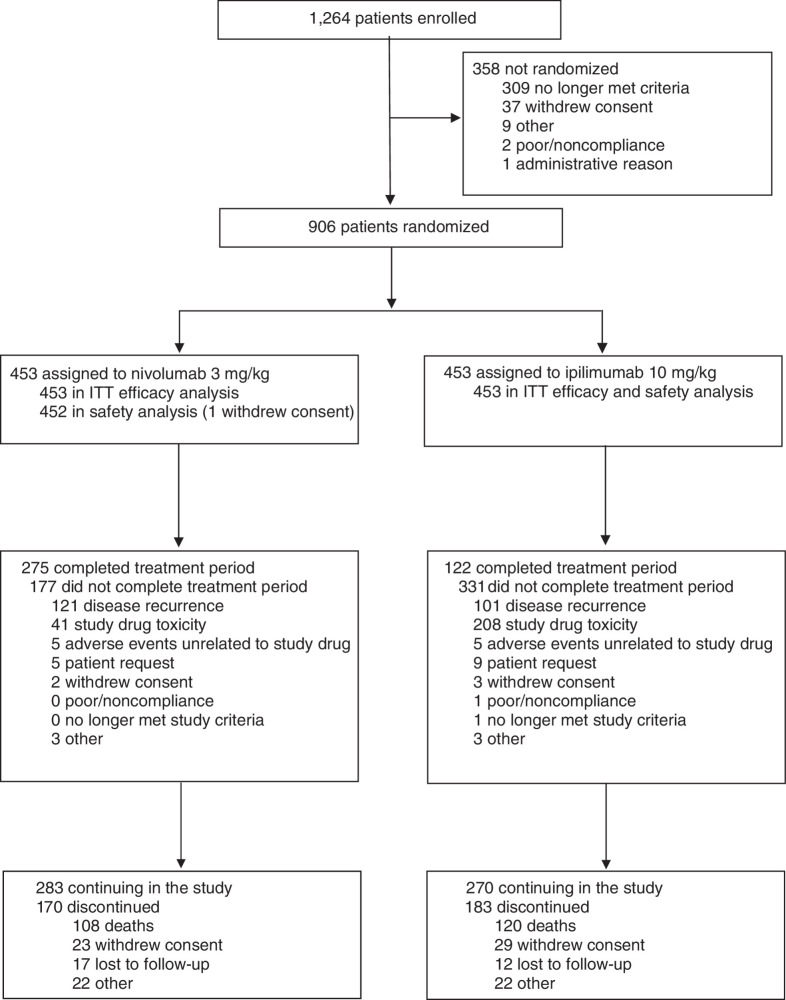
Patients and methods: Patients with resected stage IIIB-C/IV melanoma were stratified by stage and baseline programmed death cell ligand 1 (PD-L1) expression and received nivolumab 3 mg/kg every 2 weeks or ipilimumab 10 mg/kg every 3 weeks for four doses and then every 12 weeks, both intravenously for 1 year until disease recurrence, unacceptable toxicity, or withdrawal of consent. The primary endpoint was RFS.
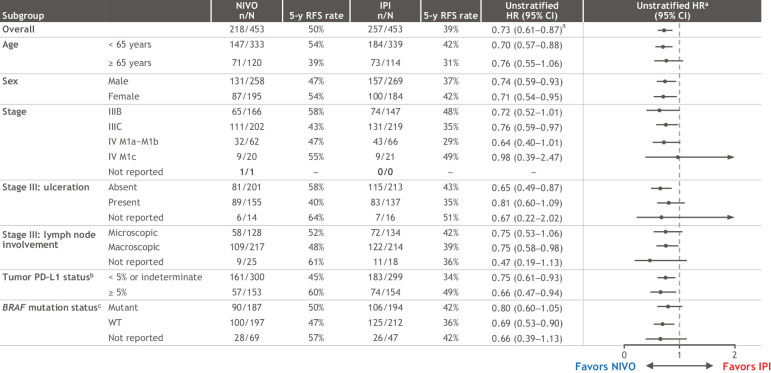
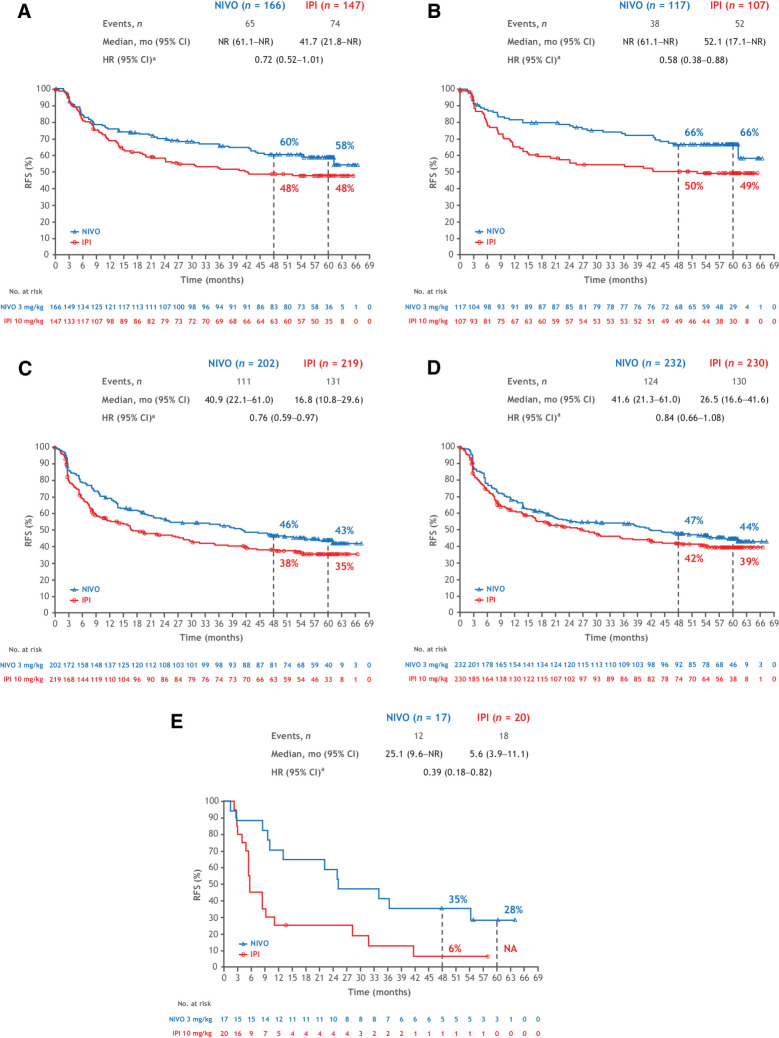
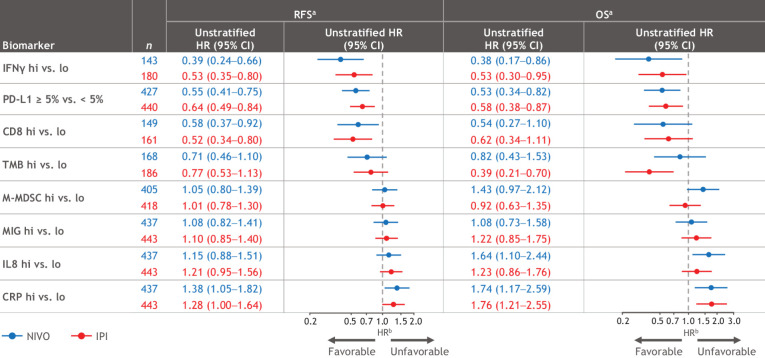
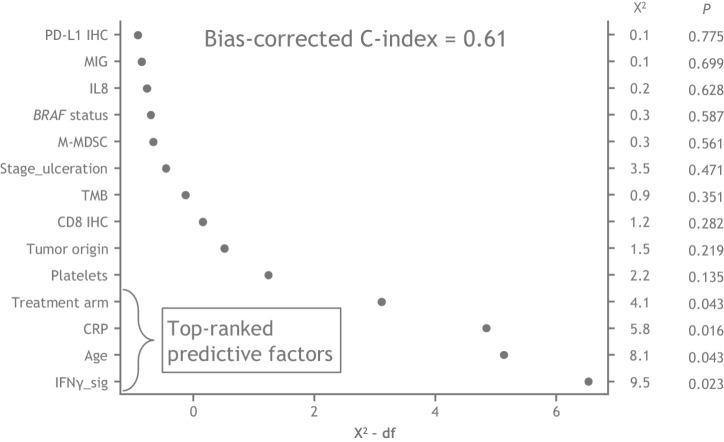
Results: At a minimum follow-up of 62 months, RFS with nivolumab remained superior to ipilimumab (HR = 0.72; 95% confidence interval, 0.60-0.86; 5-year rates of 50% vs. 39%). Five-year distant metastasis-free survival (DMFS) rates were 58% with nivolumab versus 51% with ipilimumab. Five-year overall survival (OS) rates were 76% with nivolumab and 72% with ipilimumab (75% data maturity: 228 of 302 planned events). Higher levels of tumor mutational burden (TMB), tumor PD-L1, intratumoral CD8+ T cells and IFNγ-associated gene expression signature, and lower levels of peripheral serum C-reactive protein were associated with improved RFS and OS with both nivolumab and ipilimumab, albeit with limited clinically meaningful predictive value.
Conclusions: Nivolumab is a proven adjuvant treatment for resected melanoma at high risk of recurrence, with sustained, long-term improvement in RFS and DMFS compared with ipilimumab and high OS rates. Identification of additional biomarkers is needed to better predict treatment outcome. See related commentary by Augustin and Luke, p. 3253.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
PD-1 Monotherapy Reigns Supreme in Adjuvant Melanoma…But for How Long?Clin Cancer Res. 2023 Sep 1;29(17):3253-3255. doi: 10.1158/1078-0432.CCR-23-1194. Clin Cancer Res. 2023. PMID: 37378689 Free PMC article.
References
-
- Eggermont AM, Chiarion-Sileni V, Grob JJ, Dummer R, Wolchok JD, Schmidt H, et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): a randomised, double-blind, phase 3 trial. Lancet Oncol 2015;16:522‒30. - PubMed
-
- Long GV, Hauschild A, Santinami M, Atkinson V, Mandalà M, Chiarion-Sileni V, et al. Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. N Engl J Med 2017;377:1813‒23. - PubMed
-
- Weber J, Mandala M, Del Vecchio M, Gogas HJ, Arance AM, Cowey CL, et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. N Engl J Med 2017;377:1824‒35. - PubMed
-
- Eggermont AMM, Blank CU, Mandala M, Long GV, Atkinson V, Dalle S, et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma. N Engl J Med 2018;378:1789‒1801. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
