

Dabrafenib plus trametinib in BRAFV600E-mutated rare cancers: the phase 2 ROAR trial
- PMID: 37059834
- PMCID: PMC10202803
- DOI: 10.1038/s41591-023-02321-8
Dabrafenib plus trametinib in BRAFV600E-mutated rare cancers: the phase 2 ROAR trial
Abstract
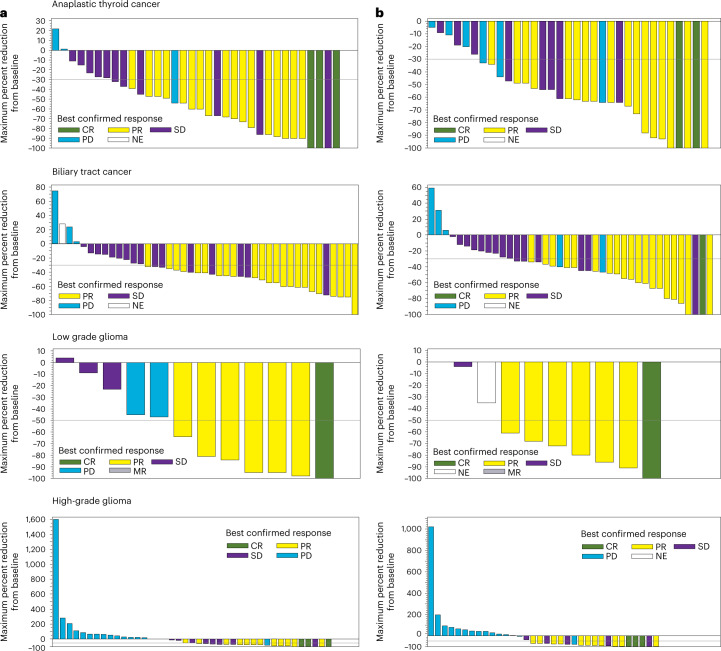
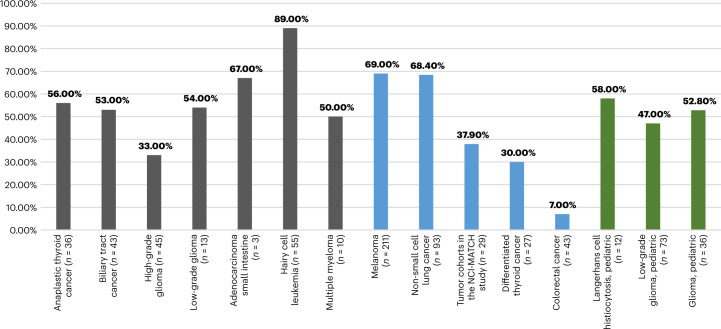
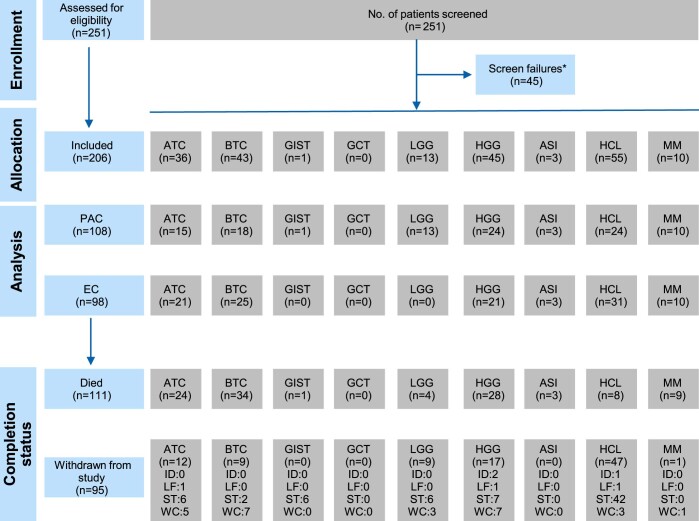
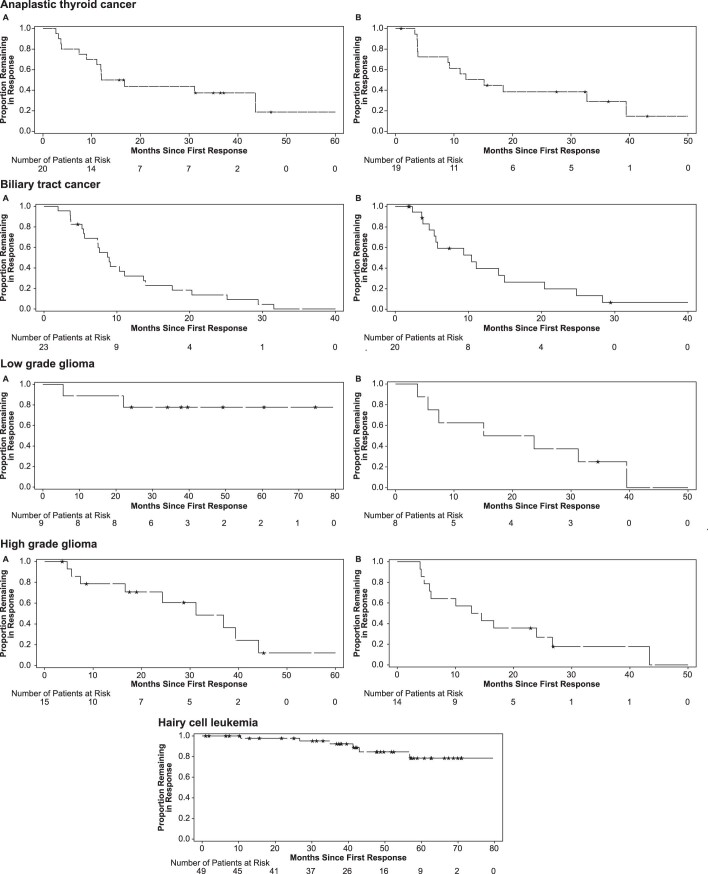
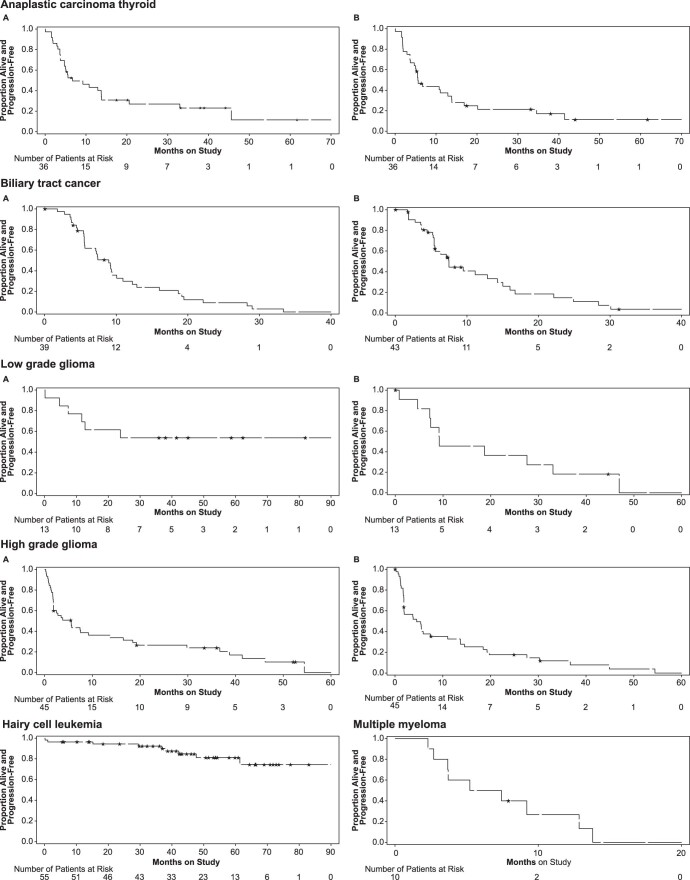
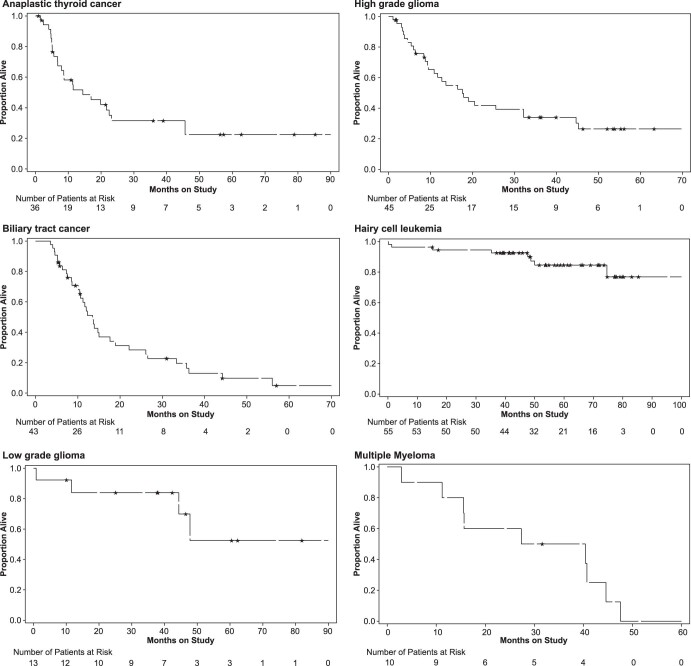
BRAFV600E alterations are prevalent across multiple tumors. Here we present final efficacy and safety results of a phase 2 basket trial of dabrafenib (BRAF kinase inhibitor) plus trametinib (MEK inhibitor) in eight cohorts of patients with BRAFV600E-mutated advanced rare cancers: anaplastic thyroid carcinoma (n = 36), biliary tract cancer (n = 43), gastrointestinal stromal tumor (n = 1), adenocarcinoma of the small intestine (n = 3), low-grade glioma (n = 13), high-grade glioma (n = 45), hairy cell leukemia (n = 55) and multiple myeloma (n = 19). The primary endpoint of investigator-assessed overall response rate in these cohorts was 56%, 53%, 0%, 67%, 54%, 33%, 89% and 50%, respectively. Secondary endpoints were median duration of response (DoR), progression-free survival (PFS), overall survival (OS) and safety. Median DoR was 14.4 months, 8.9 months, not reached, 7.7 months, not reached, 31.2 months, not reached and 11.1 months, respectively. Median PFS was 6.7 months, 9.0 months, not reached, not evaluable, 9.5 months, 5.5 months, not evaluable and 6.3 months, respectively. Median OS was 14.5 months, 13.5 months, not reached, 21.8 months, not evaluable, 17.6 months, not evaluable and 33.9 months, respectively. The most frequent (≥20% of patients) treatment-related adverse events were pyrexia (40.8%), fatigue (25.7%), chills (25.7%), nausea (23.8%) and rash (20.4%). The encouraging tumor-agnostic activity of dabrafenib plus trametinib suggests that this could be a promising treatment approach for some patients with BRAFV600E-mutated advanced rare cancers. ClinicalTrials.gov registration: NCT02034110 .
© 2023. The Author(s).
Conflict of interest statement
V.S. reports research funding from Novartis to conduct clinical trials; other grant support for clinical trials from AbbVie, Agensys, Alfasigma, Altum, Amgen, Bayer, BERG Health, Blueprint Medicines Corporation, Boston Biomedical, Boston Pharmaceuticals, Celgene Corporation, D3 Bio, Dragonfly Therapeutics, Exelixis, Fujifilm, GlaxoSmithKline, Idera Pharmaceuticals, Incyte Corporation, Inhibrx, Loxo Oncology/Eli Lilly, MedImmune, MultiVir, NanoCarrier, the National Comprehensive Cancer Network, NCI-CTEP, Novartis, PharmaMar, Pfizer, Relay Therapeutics, Roche/Genentech, Takeda, Turning Point Therapeutics, The University of Texas MD Anderson Cancer Center and Vegenics Pty. Ltd.; travel support from the American Society of Clinical Oncology (ASCO), the European Society for Medical Oncology (ESMO), Helsinn Healthcare, Incyte Corporation, Novartis and PharmaMar; consultancy or advisory board participation for Helsinn Healthcare, Incyte Corporation, Loxo Oncology/Eli Lilly, MedImmune, Novartis, QED Therapeutics, Relay Therapeutics, Daiichi-Sankyo and R-Pharm US; and other relationship with Medscape. Y.J.B. is on an advisory board or has a consulting relationship with Merck Sharp & Dohme, Merck Serono, Daiichi-Sankyo, Astellas, Alexo Oncology, Samyang Biopharm, Hanmi, Daewoong and Amgen and has received institutional grants for clinical trials from Genentech/Roche, Merck Sharp & Dohme, Merck Serono, Daiichi-Sankyo, Astellas and Amgen. A.I. has received research grant from Bayer, Bristol Myers Squibb, Roche, Novartis, Chugai, Merck, AstraZeneca, Merck Sharp & Dohme and IPSEN and is an advisory board member for Bayer, Bristol Myers Squibb, Roche, Novartis, Chugai, Merck, AstraZeneca, Merck Sharp & Dohme, IPSEN and Parthenon. F.Y.F.L.V. is part of ongoing clinical research with the Foundation STOPbraintumors.org and clinical research with sponsors including Bristol Myers Squibb, Novartis and the European Organization for Research and Treatment of Cancer; and is a faculty member of the European Society of Medical Oncology for CNS tumors, President Quality of Care Commission with the Dutch Society of Medical Oncology, Member Quality Assurance Commission of the European Organization for Research and Treatment of Cancer, and Member Educational Commission of the European Association of Neuro-Oncology. J.Y.B. has received research support and honoraria from Novartis, Roche and GlaxoSmithKline. R.J.K. has received research funds and/or drug from Novartis, AstraZeneca, Pfizer, Genentech and Teva and is a co-inventor on the National Institutes of Health patent for Moxetumomab pasudotox. D.C.C. is a consultant with Pfizer, Nektar, Merck, Exelis and Pliant. P.Y.W. has received research support from Astra Zeneca/MedImmune, Beigene, Celgene, Chimerix, Eli Lilly, Genentech/Roche, Kazia, MediciNova, Merck, Novartis, Nuvation Bio, Puma, Servier, Vascular Biogenics and VBI Vaccines; is on the advisory board of AstraZeneca, Bayer, Black Diamond, Boehringer Ingelheim, Boston Pharmaceuticals, Celularity, Chimerix, Day One Bio, Genenta, GlaxoSmithKline, Karyopharm, Merck, Mundipharma, Novartis, Novocure, Nuvation Bio, Prelude Therapeutics, Sapience, Servier, Sagimet, Vascular Biogenics and VBI Vaccines; and is an editor with UpToDate (Elsevier). S.R., A.B., P.I. and V.Q.P. are employees with Novartis and hold stock of Novartis. Z.A.W. is a consultant with Novartis, Amgen, AstraZeneca, Daiichi, Bayer, Bristol Myers Squibb, Merck, Ipsen, Gilead, Incyte, Arcus, Astellas and Molecular Templates; has received grants from Bristol Myers Squibb, Arcus and Plexxikon; and is a Data Safety and Monitoring Board member with Pfizer and Daiichi. M.J.A.J. has received financial compensation for the institute for participating in the study. J.H.M.S. is an employee with Byondis BV and a share and patent holder (oral taxanes) and employee with Modra Pharmaceuticals. E.E.F. has received honoraria for advisory role, travel grants and research grants from Amgen, Bayer, F. Hoffman-La Roche, Merck Serono, Sanofi, Pierre Fabre, Merck Sharp & Dohme, Organon, Novartis and Servier; institutional honoraria (investigator contribution in clinical trials) from Amgen, Array Biopharma, AstraZeneca, BeiGene, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Debiopharm International F. Hoffmann-La Roche, Genentech, HalioDX SAS, Hutchison MediPharma International, Janssen-Cilag, MedImmune, Menarini, Merck Health KGAA, Merck Sharp & Dohme, Merus NV, Mirati, Novartis Farmacéutica, Pfizer, Pharma Mar, Sanofi Aventis Recherche & Développement, Servier, Taiho Pharma USA; is a volunteer member of the ASCO Annual Meeting Scientific Program Committee: Developmental Therapeutics – Immunotherapy; is a speaker of the ESMO Academy; and is a coordinator of the Sociedad Española de Oncología Médica (SEOM) and MIR Section of Residents and Young Assistants. K.Y. received fees for advisory boards with Novartis, Eisai, AstraZeneca, Chugai, Takeda, Genmab and OncXerna; research support to institution from Merck Sharp & Dohme, Daiichi-Sankyo, AstraZeneca, Taiho, Pfizer, Novartis, Takeda, Chugai, Ono, Sanofi, Seattle Genetics, Eisai, Eli Lilly, Genmab, Boeringer Ingelheim, Kyowa Hakko Kirin, Nihon Kayaku and Haihe; and honoraria for lectures from Pfizer, Eisai, AstraZeneca, Eli Lilly, Takeda, Chugai, Fuji Film Pharma, Merck Sharp & Dohme, Boeringer Ingelheim, Ono and Daiichi-Sankyo. C.C.Z. has received institutional honoraria from Novartis, Bristol Myers Squibb, Merck Sharp & Dohme, Pfizer, AstraZeneca, Roche, Merck KGA, Amgen, Servier, Eli Lilly, Takeda, Daichii-Sankyo, Celgene, Halozyme and Boehringer Ingelheim and holds a patent for IMUGENE (C.F.). P.M. has received honoraria and is on advisory boards with Janssen, Celgene, Takeda, Amgen, Sanofi, Abbvie and GlaxoSmithKline. U.L. is an advisory board member and has received honoraria from Bayer, Pfizer and Novartis and has received institutional research funding from Bristol Myers Squibb, Roche, Pfizer, Incyte, Eli Lilly and GlaxoSmithKline. All remaining authors declare no competing interests.
Figures
Comment in
-
ROAR brings in a new histology-agnostic approval for rare cancers.Nat Rev Clin Oncol. 2023 Jul;20(7):425. doi: 10.1038/s41571-023-00778-7. Nat Rev Clin Oncol. 2023. PMID: 37169890 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
