

Pulmonary vein isolation by visually guided laser balloon ablation: single-center 5-year follow-up results
- PMID: 37059926
- PMCID: PMC10694101
- DOI: 10.1007/s10840-023-01544-6
Pulmonary vein isolation by visually guided laser balloon ablation: single-center 5-year follow-up results
Abstract
Background: Visually guided laser balloon (VGLB) ablation is a balloon-based treatment for atrial fibrillation (AF) that uses a titratable laser energy source to perform pulmonary vein isolation (PVI), allowing for real-time visualization of target tissue and ablation lesions through an endoscopic camera. Few long-term data on this technique are currently available. This report presents acute efficacy, procedural data, complication rates, and long-term AF-free survival up to 5 years post-ablation.
Methods: In this single-center, retrospective, observational report, 152 patients (72.4% male, mean age 60.6 ± 9.7 years, 62.5% paroxysmal AF, 598 pulmonary veins in total) treated with the first-generation VGLB system between 2014 and 2016 were included for analysis. AF ablation consisted of PVI only.
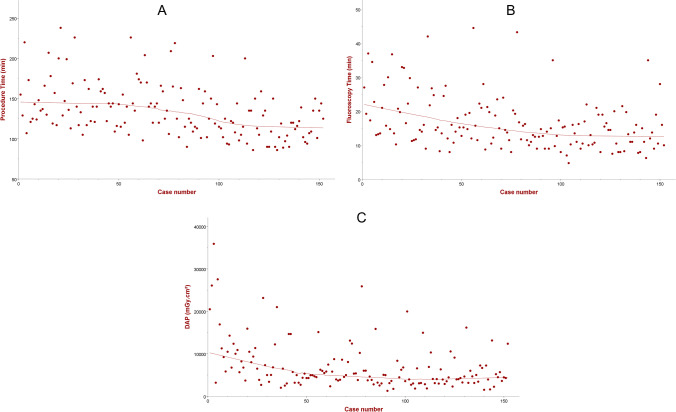
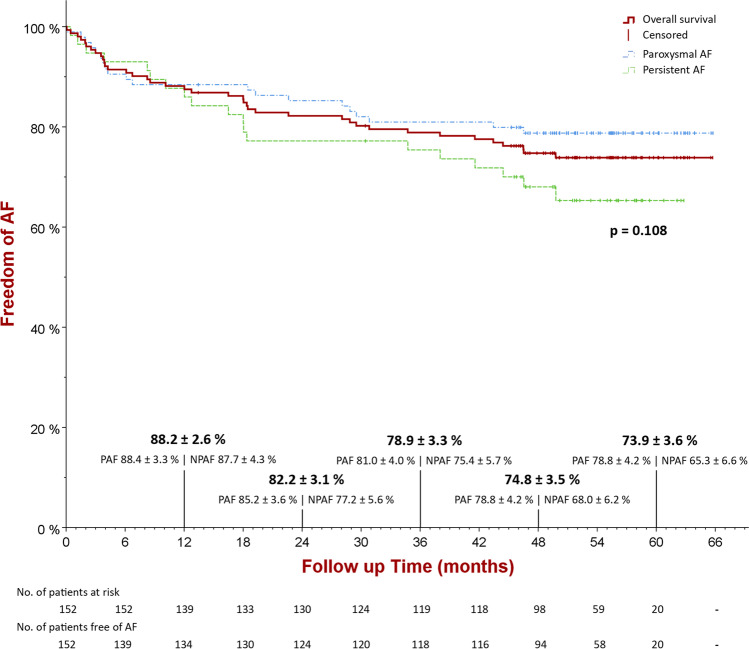
Results: Acute PVI was achieved in 98.2% of veins, with first-pass isolation in 92.5%. Procedure duration of 129 min [IQR 113-150], fluoroscopy time of 15 min [IQR 11-20], and dose area product of 5016 mGy·cm2 [IQR 3603-8711] were recorded. During a median follow-up of 51 months [IQR 45-57], 74.3% of patients remained free of AF (78.8% for paroxysmal and 65.3% for persistent AF, p = 0.108). Freedom of AF at 1, 2, 3, and 4 years follow-up was 88.2%, 82.2%, 78.9%, and 74.8%, respectively. PV reconnections were identified in only 46.9% of redo procedures. The median number of PV reconnections during redo procedures was 0 [IQR 0-2]. Anti-arrhythmic drug use was significantly reduced after ablation (p < 0.001). The most commonly reported complications were minor vascular complications (4.6%) and transient phrenic nerve paralysis (3.3%).
Conclusions: First-generation VGLB ablation demonstrated high acute isolation rates, reasonable procedure times and low complication rates. Long-term freedom from AF was 78.8% for paroxysmal AF and 65.3% for persistent AF, performing PVI only.
Keywords: Ablation; Atrial fibrillation; Laser balloon; Long-term follow-up; Pulmonary vein isolation.
© 2023. The Author(s).
Conflict of interest statement
P. Koopman has received speaker and consultant honoraria from Cardiofocus and Medtronic. J Vijgen has received speaker and consultant honoraria from Cardiofocus. All other authors: none declared.
Figures
References
-
- Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, Akar JG, Badhwar V, Brugada J, Camm J, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: executive summary. EP Europace. 2018;20(1):157–208. doi: 10.1093/europace/eux275. - DOI - PMC - PubMed
-
- Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P, Clémenty J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659–666. doi: 10.1056/NEJM199809033391003. - DOI - PubMed
-
- Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Poole JE, Noseworthy PA, Rosenberg YD, Jeffries N, Mitchell LB, et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. 2019;321(13):1261–1274. doi: 10.1001/jama.2019.0693. - DOI - PMC - PubMed
-
- Morillo CA, Verma A, Connolly SJ, Kuck KH, Nair GM, Champagne J, Sterns LD, Beresh H, Healey JS, Natale A. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of paroxysmal atrial fibrillation (RAAFT-2): a randomized trial. JAMA. 2014;311(7):692–700. doi: 10.1001/jama.2014.467. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
