

Identification of priority pathogens for aetiological diagnosis in adults with community-acquired pneumonia in China: a multicentre prospective study
- PMID: 37059987
- PMCID: PMC10103676
- DOI: 10.1186/s12879-023-08166-3
Identification of priority pathogens for aetiological diagnosis in adults with community-acquired pneumonia in China: a multicentre prospective study
Abstract
Background: Community-acquired pneumonia (CAP) is a major public health challenge worldwide. However, the aetiological and disease severity-related pathogens associated with CAP in adults in China are not well established based on the detection of both viral and bacterial agents.
Methods: A multicentre, prospective study was conducted involving 10 hospitals located in nine geographical regions in China from 2014 to 2019. Sputum or bronchoalveolar lavage fluid (BALF) samples were collected from each recruited CAP patient. Multiplex real-time PCR and bacteria culture methods were used to detect respiratory pathogens. The association between detected pathogens and CAP severity was evaluated.
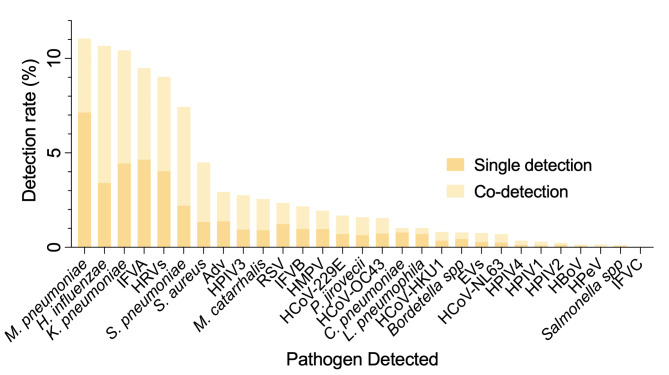
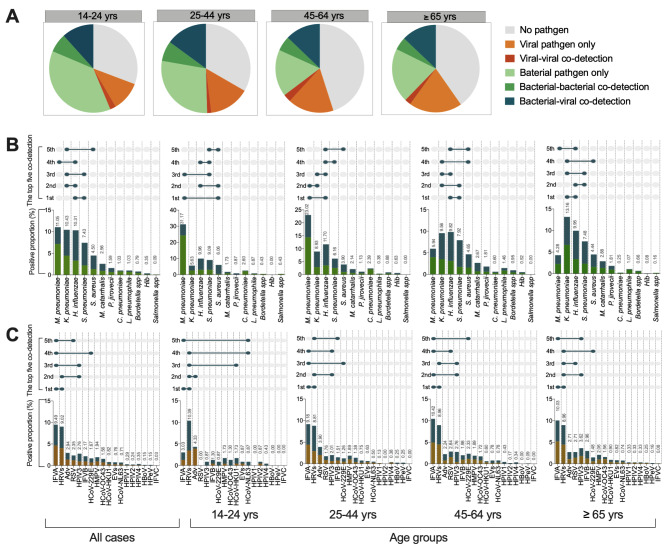
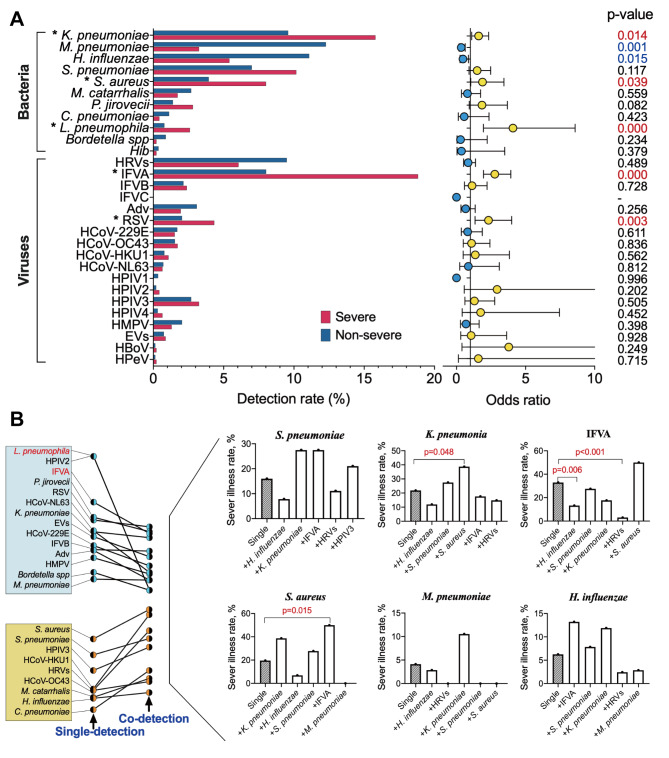
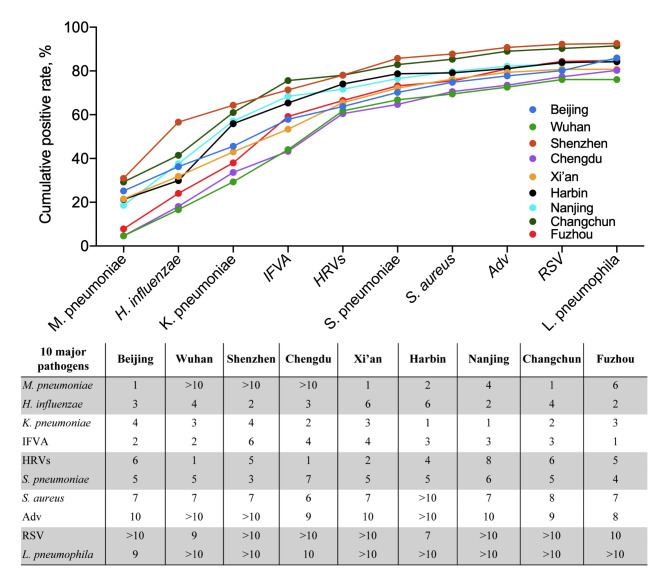
Results: Among the 3,403 recruited eligible patients, 462 (13.58%) had severe CAP, and the in-hospital mortality rate was 1.94% (66/3,403). At least one pathogen was detected in 2,054 (60.36%) patients, with two or more pathogens were co-detected in 725 patients. The ten major pathogens detected were Mycoplasma pneumoniae (11.05%), Haemophilus influenzae (10.67%), Klebsiella pneumoniae (10.43%), influenza A virus (9.49%), human rhinovirus (9.02%), Streptococcus pneumoniae (7.43%), Staphylococcus aureus (4.50%), adenovirus (2.94%), respiratory syncytial viruses (2.35%), and Legionella pneumophila (1.03%), which accounted for 76.06-92.52% of all positive detection results across sampling sites. Klebsiella pneumoniae (p < 0.001) and influenza viruses (p = 0.005) were more frequently detected in older patients, whereas Mycoplasma pneumoniae was more frequently detected in younger patients (p < 0.001). Infections with Klebsiella pneumoniae, Staphylococcus aureus, influenza viruses and respiratory syncytial viruses were risk factors for severe CAP.
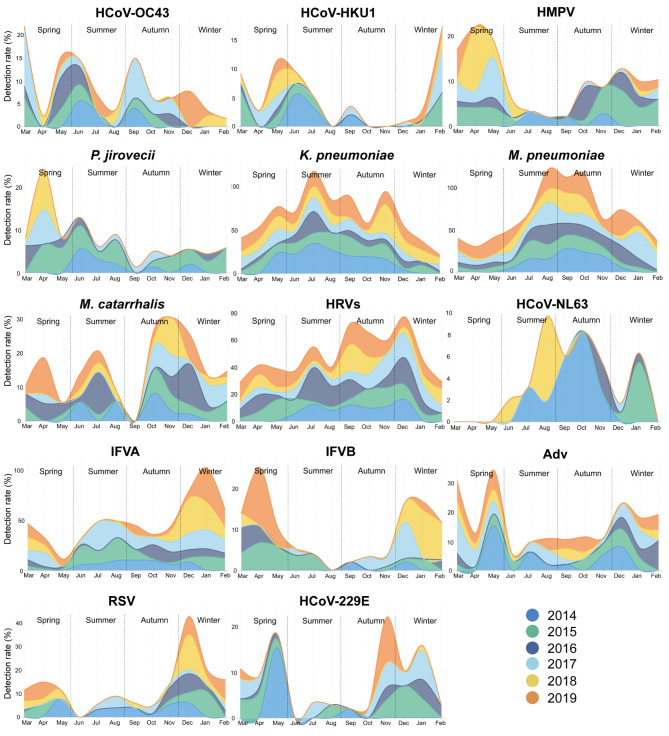
Conclusions: The major respiratory pathogens causing CAP in adults in China were different from those in USA and European countries, which were consistent across different geographical regions over study years. Given the detection rate of pathogens and their association with severe CAP, we propose to include the ten major pathogens as priorities for clinical pathogen screening in China.
Keywords: Aetiology; Community-acquired pneumonia; Priority screening pathogens; Risk factor; Severe infection.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interest.
Figures
Similar articles
-
Infection and co-infection patterns of community-acquired pneumonia in patients of different ages in China from 2009 to 2020: a national surveillance study.Lancet Microbe. 2023 May;4(5):e330-e339. doi: 10.1016/S2666-5247(23)00031-9. Epub 2023 Mar 28. Lancet Microbe. 2023. PMID: 37001538
-
[Pay attention to new evolution trends in the etiology of community-acquired pneumonia in adults].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Jun 12;47(6):576-581. doi: 10.3760/cma.j.cn112147-20231024-00264. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38858211 Chinese.
-
Diagnosis of atypical pathogens in patients hospitalized with community-acquired respiratory infection.Scand J Infect Dis. 2004;36(4):269-73. doi: 10.1080/00365540410020127. Scand J Infect Dis. 2004. PMID: 15198183
-
Childhood community-acquired pneumonia.Eur J Pediatr. 2024 Mar;183(3):1129-1136. doi: 10.1007/s00431-023-05366-6. Epub 2023 Dec 19. Eur J Pediatr. 2024. PMID: 38112800 Free PMC article. Review.
-
Community-acquired pneumonia related to intracellular pathogens.Intensive Care Med. 2016 Sep;42(9):1374-86. doi: 10.1007/s00134-016-4394-4. Epub 2016 Jun 8. Intensive Care Med. 2016. PMID: 27276986 Review.
Cited by
-
The Clinical Application Value of a Novel Chip in the Detection of Pathogens in Adult Pneumonia: A Multi-Centre Prospective Study in China.Infect Drug Resist. 2024 Nov 5;17:4843-4852. doi: 10.2147/IDR.S483256. eCollection 2024. Infect Drug Resist. 2024. PMID: 39524976 Free PMC article.
-
Clinical and prognostic relevance of Mycoplasma felis PCR detection in feline lower respiratory tract disease.J Feline Med Surg. 2024 Dec;26(12):1098612X241297870. doi: 10.1177/1098612X241297870. J Feline Med Surg. 2024. PMID: 39718117 Free PMC article.
-
A new pathogen pattern of acute respiratory tract infections in primary care after COVID-19 pandemic: a multi-center study in southern China.BMC Infect Dis. 2025 Jan 21;25(1):98. doi: 10.1186/s12879-025-10500-w. BMC Infect Dis. 2025. PMID: 39838340 Free PMC article.
-
The impact of the COVID-19 pandemic on Staphylococcus aureus infections in pediatric patients admitted with community acquired pneumonia.Sci Rep. 2024 Jul 8;14(1):15737. doi: 10.1038/s41598-024-66071-4. Sci Rep. 2024. PMID: 38977804 Free PMC article.
-
Comparison of the clinical characteristics in parents and their children in a series of family clustered Mycoplasma pneumoniae infections.BMC Pulm Med. 2024 Mar 4;24(1):107. doi: 10.1186/s12890-024-02922-0. BMC Pulm Med. 2024. PMID: 38439032 Free PMC article.
References
-
- World Health Organization. The top 10 causes of death. 2019. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
-
- Zhou F, Wang Y, Liu Y, Liu X, Gu L, Zhang X et al. Disease severity and clinical outcomes of community-acquired pneumonia caused by non-influenza respiratory viruses in adults: a multicentre prospective registry study from the CAP-China Network. Eur Respir J. 2019; 54(2). - PubMed
-
- GBD 2017 Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of Disease Study 2017. Lancet. 2018;392:1736–88. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- 2020B1111170014/the Guangdong Scientific and Technological Foundation
- 2017ZX10103004/the National Major Science & Technology Project for Control and Prevention of Major Infectious Diseases in China
- 2021-I2M-1-038/Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (CIFMS)
- 2019PT31002/the Nonprofit Central Research Institute Fund of Chinese Academy of Medical Sciences
- Z190017/Beijing Municipal Natural Science Foundation
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
