

Effects of magnesium sulfate on periarticular infiltration analgesia in total knee arthroplasty: a prospective, double-blind, randomized controlled trial
- PMID: 37060089
- PMCID: PMC10105472
- DOI: 10.1186/s13018-023-03790-w
Effects of magnesium sulfate on periarticular infiltration analgesia in total knee arthroplasty: a prospective, double-blind, randomized controlled trial
Abstract
Background: To investigate whether adding magnesium sulfate to a periarticular infiltration analgesia (PIA) cocktail could improve pain control and functional outcomes in patients undergoing total knee arthroplasty (TKA).
Methods: Ninety patients were randomly assigned to the magnesium sulfate and control groups, with 45 patients in each group. In the magnesium sulfate group, patients were given a periarticular infusion of a cocktail of analgesics consisting of epinephrine, ropivacaine, magnesium sulfate, and dexamethasone. The control group received no magnesium sulfate. The primary outcomes consisted of visual analogue scale (VAS) pain scores, postoperative morphine hydrochloride consumption for rescue analgesia, and time to first rescue analgesia. Secondary outcomes were postoperative inflammatory biomarkers (IL-6 and CRP), postoperative length of stay, and knee functional recovery (assessed by knee range of motion, quadriceps strength, daily mobilization distance, and time to first straight-leg raising). Tertiary outcomes included the postoperative swelling ratio and complication rates.
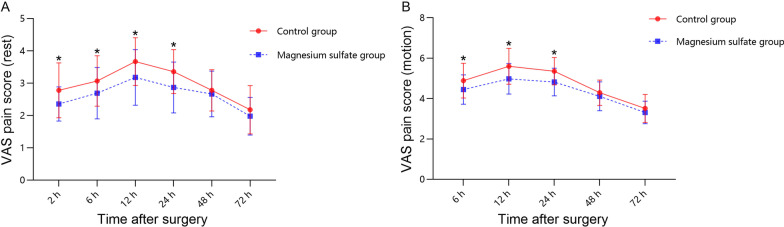
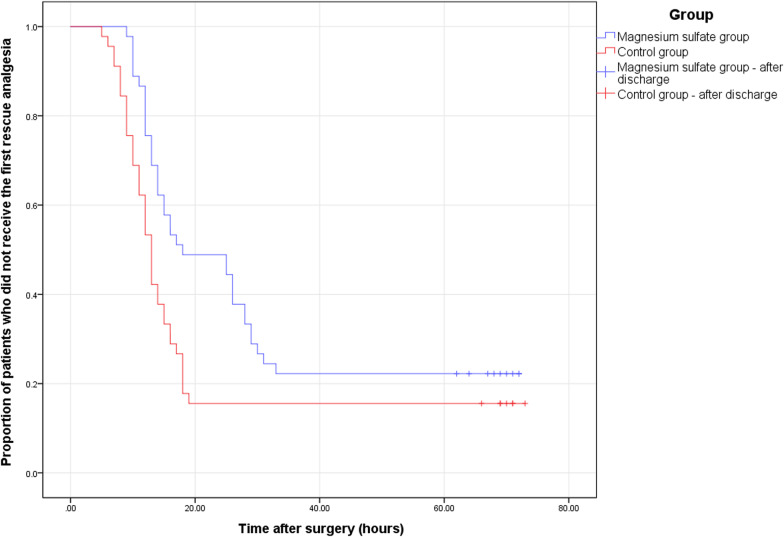
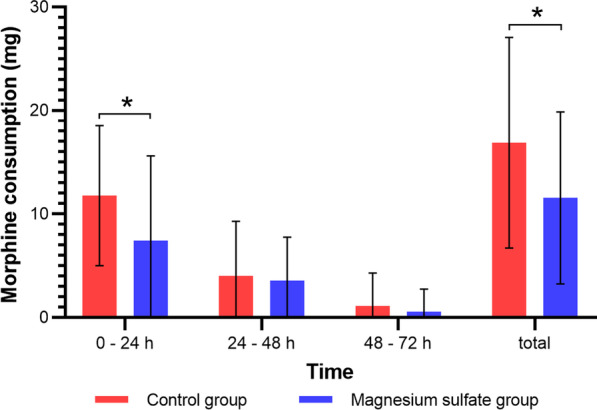
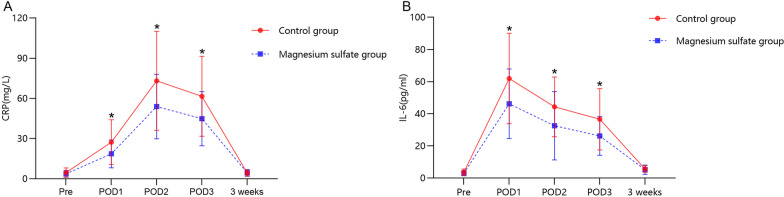
Results: Within 24 h of surgery, patients in the magnesium sulfate group had markedly lower VAS pain scores during motion and at rest. After the addition of magnesium sulfate, the analgesic effect was dramatically prolonged, leading to a reduction in morphine dosage within 24 h and the total morphine dosage postoperatively. Postoperative inflammatory biomarker levels were significantly reduced in the magnesium sulfate group compared with the control. There were no considerable differences between the groups in terms of the postoperative length of stay and knee functional recovery. Both groups had similar postoperative swelling ratios and incidences of complications.
Conclusions: The addition of magnesium sulfate to the analgesic cocktail for PIA can prolong postoperative analgesia, decrease the consumption of opioids, and effectively alleviate early postoperative pain after TKA.
Trial registration: Chinese Clinical Trial Registry, ChiCTR2200056549. Registered on 7 February 2022, https://www.chictr.org.cn/showproj.aspx?proj=151489 .
Keywords: Cocktail; Magnesium sulfate; Pain; Periarticular infiltration analgesia; Total knee arthroplasty.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Li D, Alqwbani M, Wang Q, Liao R, Yang J, Kang P. Efficacy of adductor canal block combined with additional analgesic methods for postoperative analgesia in total knee arthroplasty: a prospective, double-blind, randomized controlled study. J Arthroplasty. 2020;35(12):3554–3562. doi: 10.1016/j.arth.2020.06.060. - DOI - PubMed
-
- Kopp SL, Børglum J, Buvanendran A, Horlocker TT, Ilfeld BM, Memtsoudis SG, Neal JM, Rawal N, Wegener JT. Anesthesia and analgesia practice pathway options for total knee arthroplasty: an evidence-based review by the american and european societies of regional anesthesia and pain medicine. Reg Anesth Pain Med. 2017;42(6):683–697. doi: 10.1097/AAP.0000000000000673. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
