

N-terminal brain natriuretic peptide, cardiac troponin-I, and point-of-care ultrasound in dogs with cardiac and noncardiac causes of nonhemorrhagic ascites
- PMID: 37060291
- PMCID: PMC10229338
- DOI: 10.1111/jvim.16702
N-terminal brain natriuretic peptide, cardiac troponin-I, and point-of-care ultrasound in dogs with cardiac and noncardiac causes of nonhemorrhagic ascites
Abstract
Background: Nonhemorrhagic ascites (NHA) can be caused by cardiac diseases (cNHA) and noncardiac diseases (ncNHA). N-terminal brain natriuretic peptide (NT-proBNP), cardiac troponin-I (cTnI), and point-of-care ultrasound (POCUS) may differentiate between cNHA and ncNHA.
Hypothesis/objectives: We compared NT-proBNP and cTnI concentrations as well as POCUS findings in dogs presented with cNHA and ncNHA.
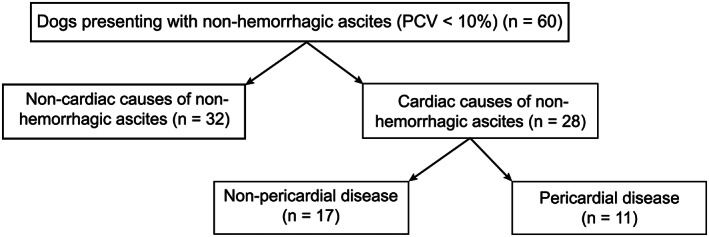
Animals: Dogs (n = 60) were enrolled based on identification of NHA with an effusion packed cell volume < 10%.
Methods: Blood samples were collected and POCUS was performed on all dogs. Dogs were diagnosed with cNHA (n = 28) or ncNHA (n = 32) based on echocardiography. The cNHA group was subdivided into cardiac non-pericardial disease (n = 17) and pericardial disease (n = 11).
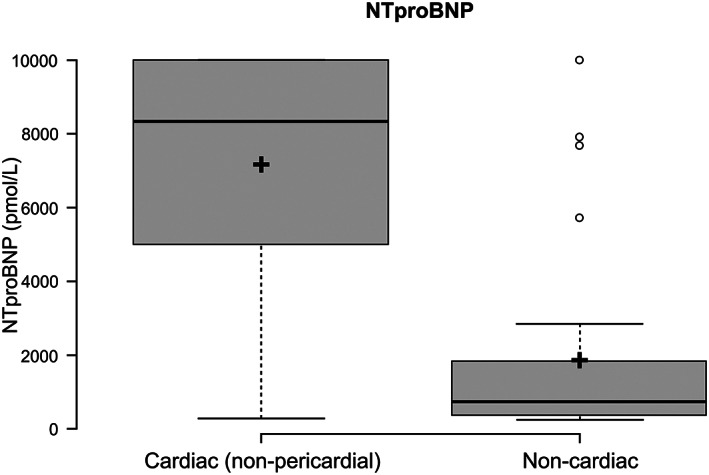
Results: The NT-proBNP concentration (median; range pmol/L) was significantly higher in the cNHA group (4510; 250-10 000) compared to the ncNHA group (739.5; 250-10 000; P = .01), with a sensitivity of 53.8% and specificity of 85.7% using a cut-off of 4092 pmol/L. The NT-proBNP concentrations were significantly higher in the cardiac non-pericardial disease group (8339; 282-10 000) compared with the pericardial disease group (692.5; 250-4928; P = .002). A significant difference in cTnI concentration (median; range ng/L) between the cNHA group (300; 23-112 612) and ncNHA group (181; 17-37 549) was not detected (P = .41). A significantly higher number of dogs had hepatic venous and caudal vena cava distension in the cNHA group compared to the ncNHA group, respectively (18/28 vs 3/29, P < .0001 and 13/27 vs 2/29, P < .001). Gall bladder wall edema was not significantly different between groups (4/28 vs 3/29, P = .74).
Conclusions and clinical importance: NT-proBNP concentration and POCUS help distinguish between cNHA and ncNHA.
Keywords: BNP; canine; congestive heart failure; echocardiography.
© 2023 The Authors. Journal of Veterinary Internal Medicine published by Wiley Periodicals LLC on behalf of American College of Veterinary Internal Medicine.
Conflict of interest statement
Authors declare no conflict of interest.
Figures


Similar articles
-
[NT-proBNP as a diagnostic marker in dogs with dyspnea and in asymptomatic dogs with heart murmur].Tierarztl Prax Ausg K Kleintiere Heimtiere. 2012;40(3):171-9. Tierarztl Prax Ausg K Kleintiere Heimtiere. 2012. PMID: 22688794 German.
-
Relationship of plasma N-terminal pro-brain natriuretic peptide concentrations to heart failure classification and cause of respiratory distress in dogs using a 2nd generation ELISA assay.J Vet Intern Med. 2015 Jan;29(1):171-9. doi: 10.1111/jvim.12472. Epub 2014 Oct 10. J Vet Intern Med. 2015. PMID: 25308881 Free PMC article.
-
Distinguishing cardiac and noncardiac dyspnea in 48 dogs using plasma atrial natriuretic factor, B-type natriuretic factor, endothelin, and cardiac troponin-I.J Vet Intern Med. 2007 Mar-Apr;21(2):238-42. doi: 10.1892/0891-6640(2007)21[238:dcandi]2.0.co;2. J Vet Intern Med. 2007. PMID: 17427383
-
Biomarkers for differentiation of causes of respiratory distress in dogs and cats: Part 1--Cardiac diseases and pulmonary hypertension.J Vet Emerg Crit Care (San Antonio). 2015 May-Jun;25(3):311-29. doi: 10.1111/vec.12318. J Vet Emerg Crit Care (San Antonio). 2015. PMID: 26040814 Review.
-
Use of B-Type Natriuretic Peptide (BNP) and N-Terminal proBNP (NT-proBNP) as Diagnostic Tests in Adults With Suspected Heart Failure: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 May 6;21(2):1-125. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34055110 Free PMC article.
References
-
- Walter J. Abdominal enlargement. In: Ettinger SJ, Feldman EC, Cote E, eds. Textbook of Veterinary Internal Medicine: Diseases of the Dog and Cat. Vol 1. 8th ed. St. Louis, MO: Elsevier; 2017:78‐81.
-
- Valenciano AC, Rizzi TE. Abdominal, thoracic, and pericardial effusions. In: Valenciano AC, Cowell RL, eds. Cowell and Tyler's Diagnostic Cytology and Hematology of the Dog and Cat. 5th ed. St. Louis, MO: Elsevier; 2020:229‐246.
-
- Dempsey SM, Ewing PJ. A review of the pathophysiology, classification, and analysis of canine and feline cavitary effusions. J Am Anim Hosp Assoc. 2011;47(1):1‐11. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
