

Multiparametric dynamic whole-body PSMA PET/CT using [68Ga]Ga-PSMA-11 and [18F]PSMA-1007
- PMID: 37060394
- PMCID: PMC10105814
- DOI: 10.1186/s13550-023-00981-8
Multiparametric dynamic whole-body PSMA PET/CT using [68Ga]Ga-PSMA-11 and [18F]PSMA-1007
Abstract
Background: Routine prostate-specific membrane antigen (PSMA) positron emission tomography (PET) performed for primary staging or restaging of prostate cancer patients is usually done as a single static image acquisition 60 min after tracer administration. In this study, we employ dynamic whole-body (D-WB) PET imaging to compare the pharmacokinetics of [68Ga]Ga-PSMA-11 and [18F]PSMA-1007 in various tissues and lesions, and to assess whether Patlak parametric images are quantitative and improve lesion detection and image readability.
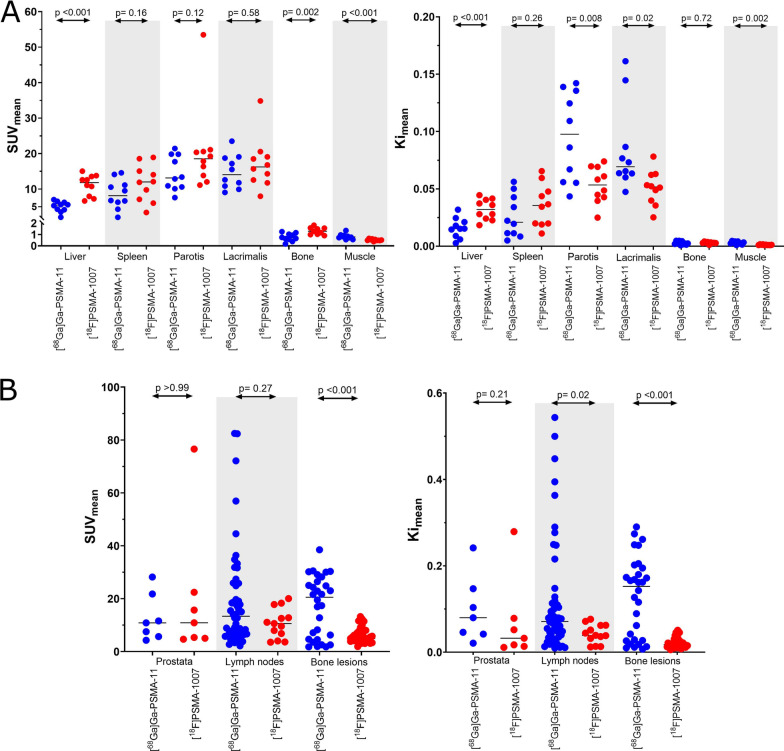
Methods: Twenty male patients with prostate cancer were examined using a D-WB PSMA PET protocol. Ten patients were scanned with [68Ga]Ga-PSMA-11 and ten with [18F]PSMA-1007. Kinetic analyses were made using time-activity curves (TACs) extracted from organs (liver, spleen, bone, and muscle) and lesions. For each patient, three images were produced: SUV + Patlak parametric images (Ki and DV). All images were reviewed visually to compare lesion detection, image readability was quantified using target-to-background ratios (TBR), and Ki and DV values were compared.
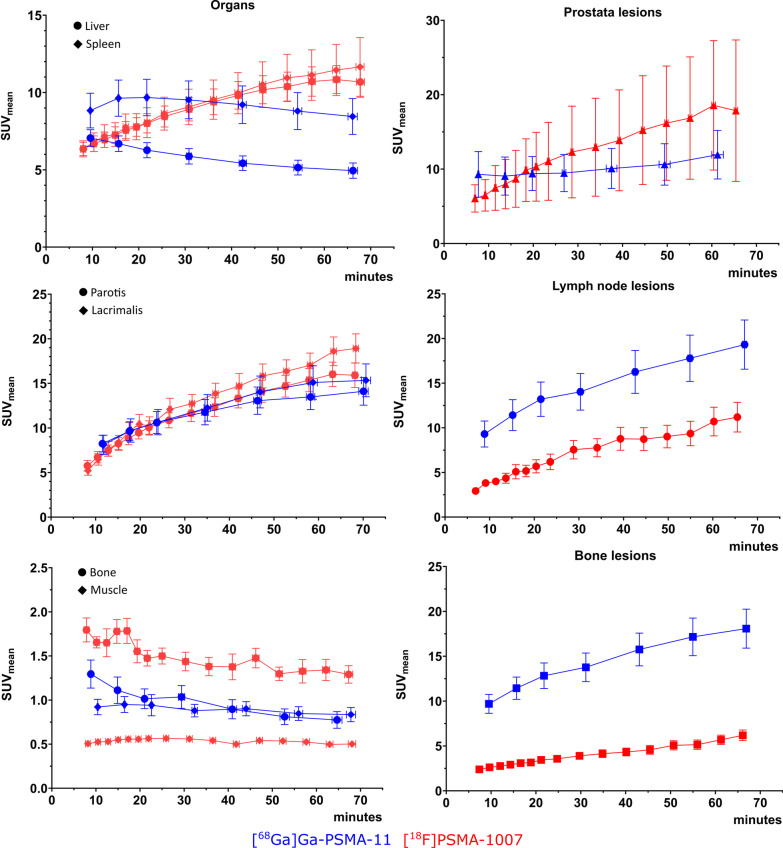
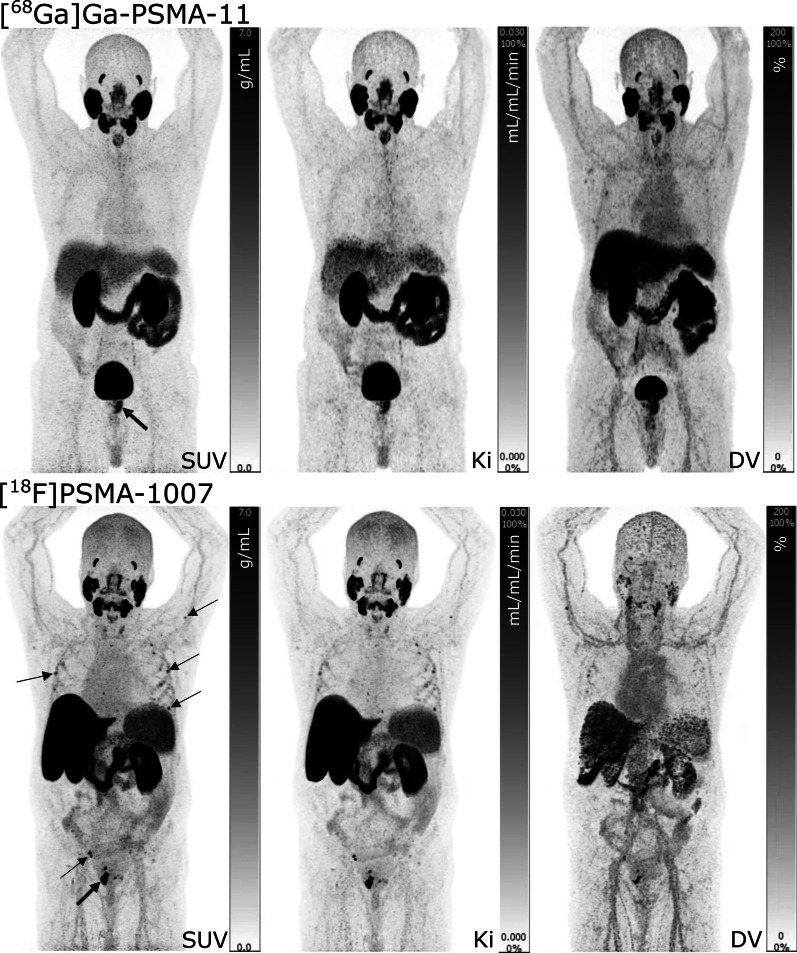
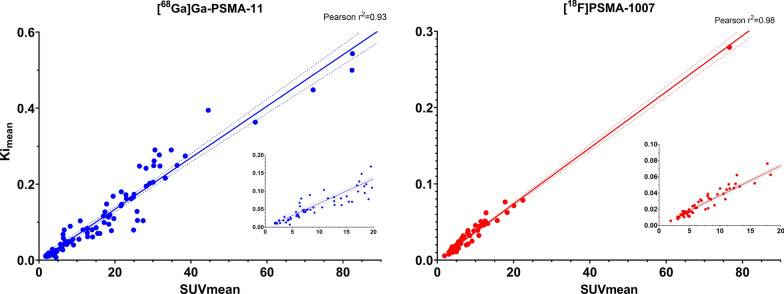
Results: The two PSMA tracers exhibited markedly different pharmacokinetics in organs: reversible for [68Ga]Ga-PSMA-11 and irreversible for [18F]PSMA-1007. For both tracers, lesions kinetics were best described by an irreversible model. All parametric images were of good visual quality using both radiotracers. In general, Ki images were characterized by reduced vascular signal and increased lesion TBR compared with SUV images. No additional malignant lesions were identified on the parametric images.
Conclusion: D-WB PET/CT is feasible for both PSMA tracers allowing for direct reconstruction of parametric Ki images. The use of multiparametric PSMA images increased TBR but did not lead to the detection of more lesions. For quantitative whole-body Ki imaging, [18F]PSMA-1007 should be preferred over [68Ga]Ga-PSMA-11 due to its irreversible kinetics in organs and lesions.
Keywords: Dynamic whole-body PET; Oncology; PSMA; Parametric imaging; Patlak; Prostate cancer.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Comparison of parametric imaging and SUV imaging with [68 Ga]Ga-PSMA-11 using dynamic total-body PET/CT in prostate cancer.Eur J Nucl Med Mol Imaging. 2024 Jan;51(2):568-580. doi: 10.1007/s00259-023-06456-1. Epub 2023 Oct 4. Eur J Nucl Med Mol Imaging. 2024. PMID: 37792025
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Kinetic modeling and parametric imaging of 18 F-PSMA-11: An evaluation based on total-body dynamic positron emission tomography scans.Med Phys. 2024 Jan;51(1):156-166. doi: 10.1002/mp.16876. Epub 2023 Dec 3. Med Phys. 2024. PMID: 38043120
-
68Ga-Labeled Prostate-specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography for Prostate Cancer: A Systematic Review and Meta-analysis.Eur Urol Focus. 2018 Sep;4(5):686-693. doi: 10.1016/j.euf.2016.11.002. Epub 2016 Nov 15. Eur Urol Focus. 2018. PMID: 28753806
-
Comparing the Staging/Restaging Performance of 68Ga-Labeled Prostate-Specific Membrane Antigen and 18F-Choline PET/CT in Prostate Cancer: A Systematic Review and Meta-analysis.Clin Nucl Med. 2019 May;44(5):365-376. doi: 10.1097/RLU.0000000000002526. Clin Nucl Med. 2019. PMID: 30888999
Cited by
-
Assessing dynamic metabolic heterogeneity in prostate cancer patients via total-body [68Ga]Ga-PSMA-11 PET/CT imaging: quantitative analysis of [68Ga]Ga-PSMA-11 uptake in pathological lesions and normal organs.Eur J Nucl Med Mol Imaging. 2024 Feb;51(3):896-906. doi: 10.1007/s00259-023-06475-y. Epub 2023 Oct 27. Eur J Nucl Med Mol Imaging. 2024. PMID: 37889299
-
Comparison of parametric imaging and SUV imaging with [68 Ga]Ga-PSMA-11 using dynamic total-body PET/CT in prostate cancer.Eur J Nucl Med Mol Imaging. 2024 Jan;51(2):568-580. doi: 10.1007/s00259-023-06456-1. Epub 2023 Oct 4. Eur J Nucl Med Mol Imaging. 2024. PMID: 37792025
-
Combined whole-body dynamic and static PET/CT with low-dose [18F]PSMA-1007 in prostate cancer patients.Eur J Nucl Med Mol Imaging. 2024 Jun;51(7):2137-2150. doi: 10.1007/s00259-024-06620-1. Epub 2024 Jan 30. Eur J Nucl Med Mol Imaging. 2024. PMID: 38286936 Free PMC article.
-
Direct Patlak Reconstruction of [68Ga]Ga-PSMA PET for the Evaluation of Primary Prostate Cancer Prior Total Prostatectomy: Results of a Pilot Study.Int J Mol Sci. 2023 Sep 5;24(18):13677. doi: 10.3390/ijms241813677. Int J Mol Sci. 2023. PMID: 37761975 Free PMC article.
-
Parametric net influx rate imaging of 68Ga-DOTATATE in patients with neuroendocrine tumors: assessment of lesion detectability.Ann Nucl Med. 2024 Jul;38(7):483-492. doi: 10.1007/s12149-024-01922-8. Epub 2024 Apr 4. Ann Nucl Med. 2024. PMID: 38573411
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
