

Anthracycline-containing and taxane-containing chemotherapy for early-stage operable breast cancer: a patient-level meta-analysis of 100 000 women from 86 randomised trials
- PMID: 37061269
- PMCID: PMC11023015
- DOI: 10.1016/S0140-6736(23)00285-4
Anthracycline-containing and taxane-containing chemotherapy for early-stage operable breast cancer: a patient-level meta-analysis of 100 000 women from 86 randomised trials
Abstract
Background: Anthracycline-taxane chemotherapy for early-stage breast cancer substantially improves survival compared with no chemotherapy. However, concerns about short-term and long-term side-effects of anthracyclines have led to increased use of taxane chemotherapy without anthracycline, which could compromise efficacy. We aimed to better characterise the benefits and risks of including anthracycline, and the comparative benefits of different anthracycline-taxane regimens.
Methods: We did an individual patient-level meta-analysis of randomised trials comparing taxane regimens with versus without anthracycline, and updated our previous meta-analysis of anthracycline regimens with versus without taxane, as well as analysing 44 trials in six related comparisons. We searched databases, including MEDLINE, Embase, the Cochrane Library, and meeting abstracts to identify trials assessing anthracycline and taxane chemotherapy. Adjuvant or neoadjuvant trials were eligible if they began before Jan 1, 2012. Primary outcomes were breast cancer recurrence and cause-specific mortality. Log-rank analyses yielded first-event rate ratios (RRs) and CIs.
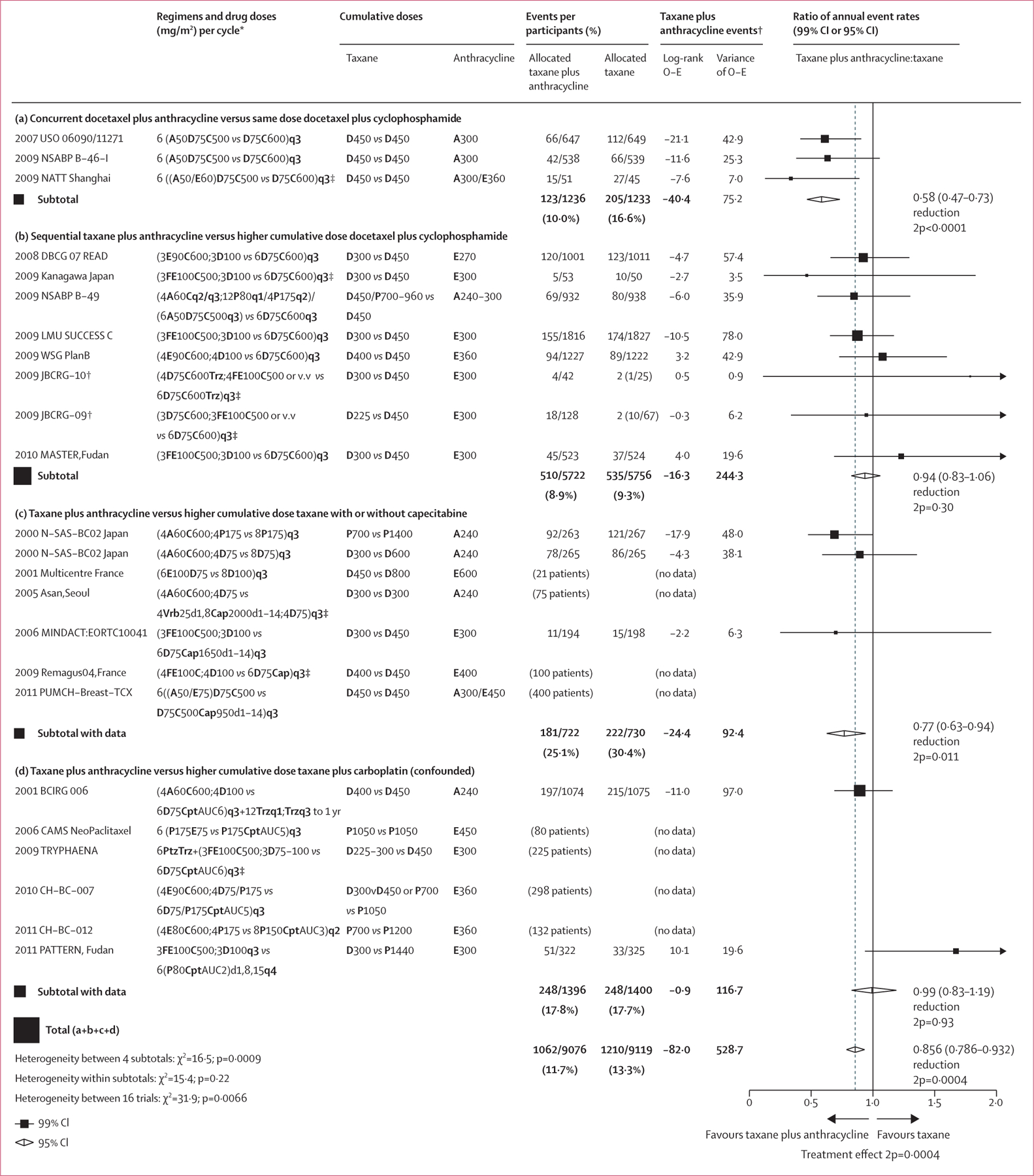
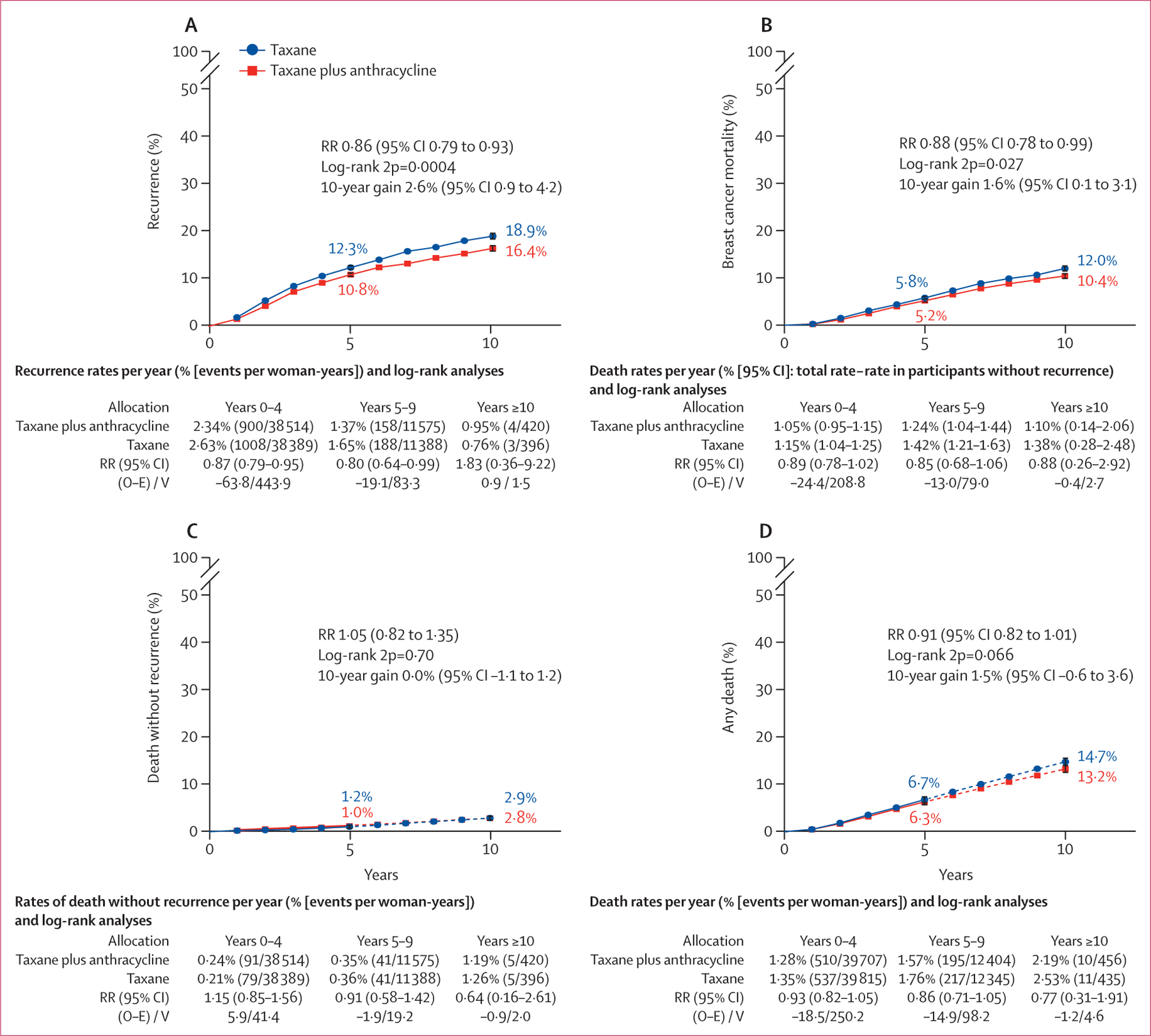
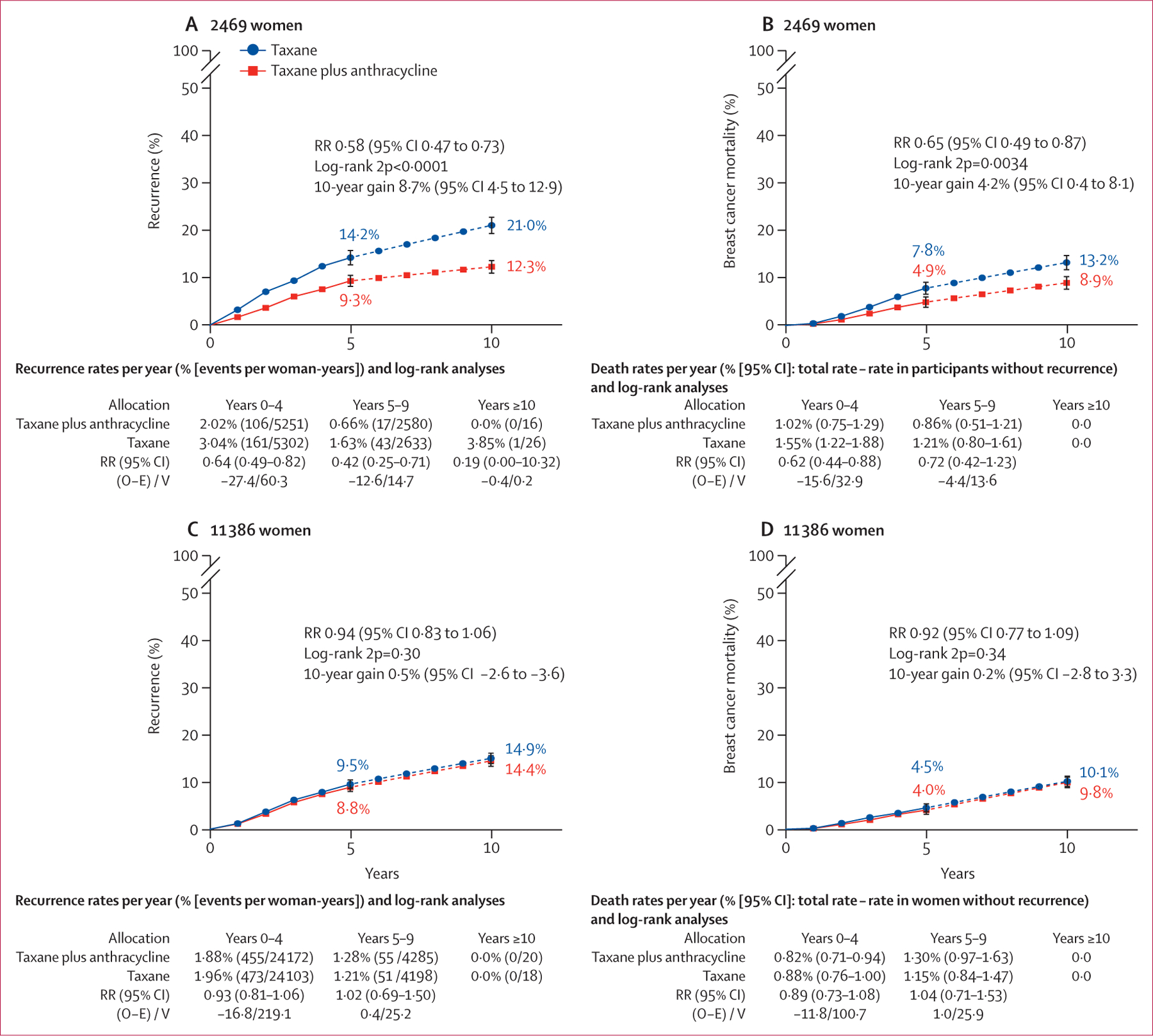
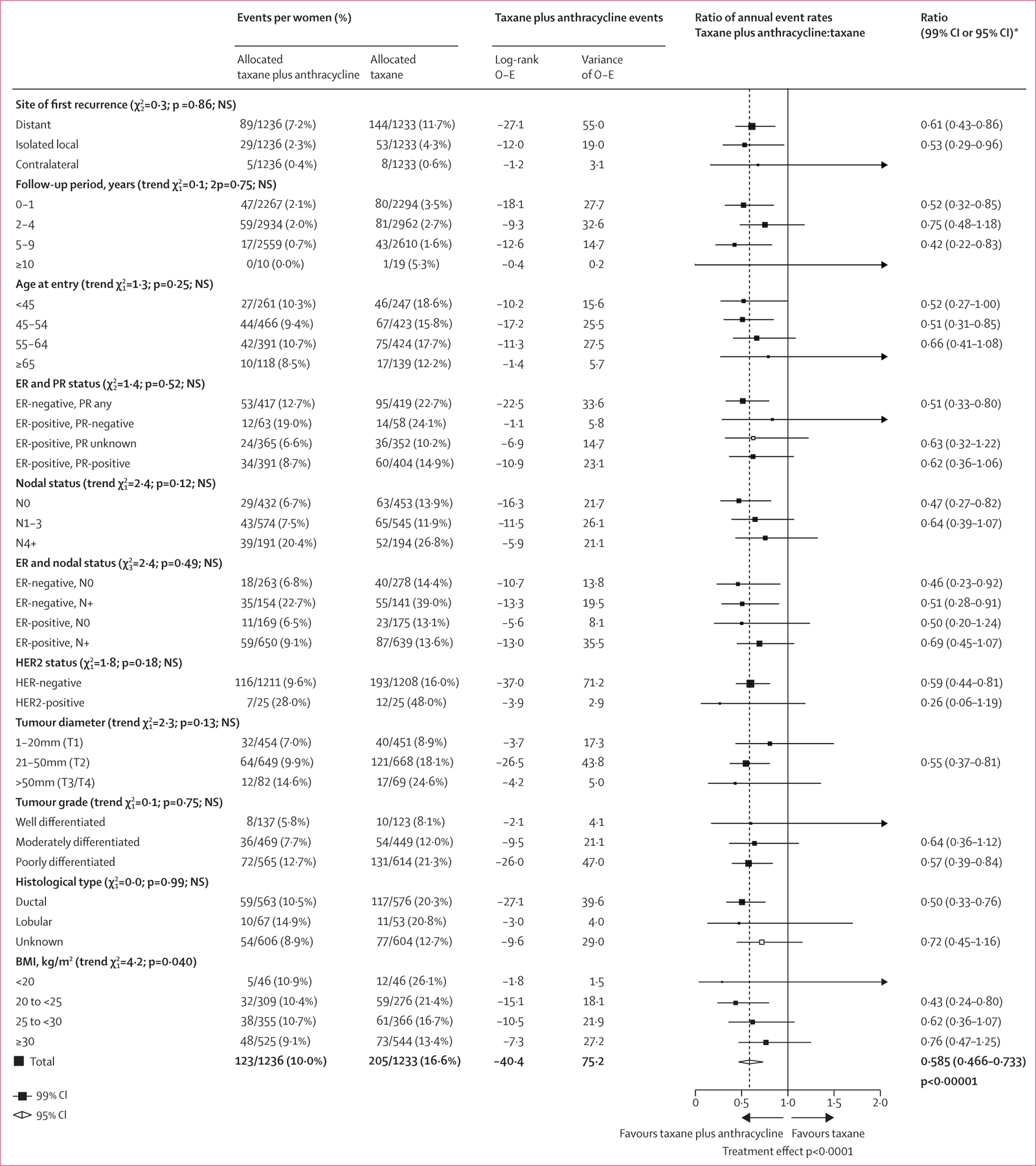
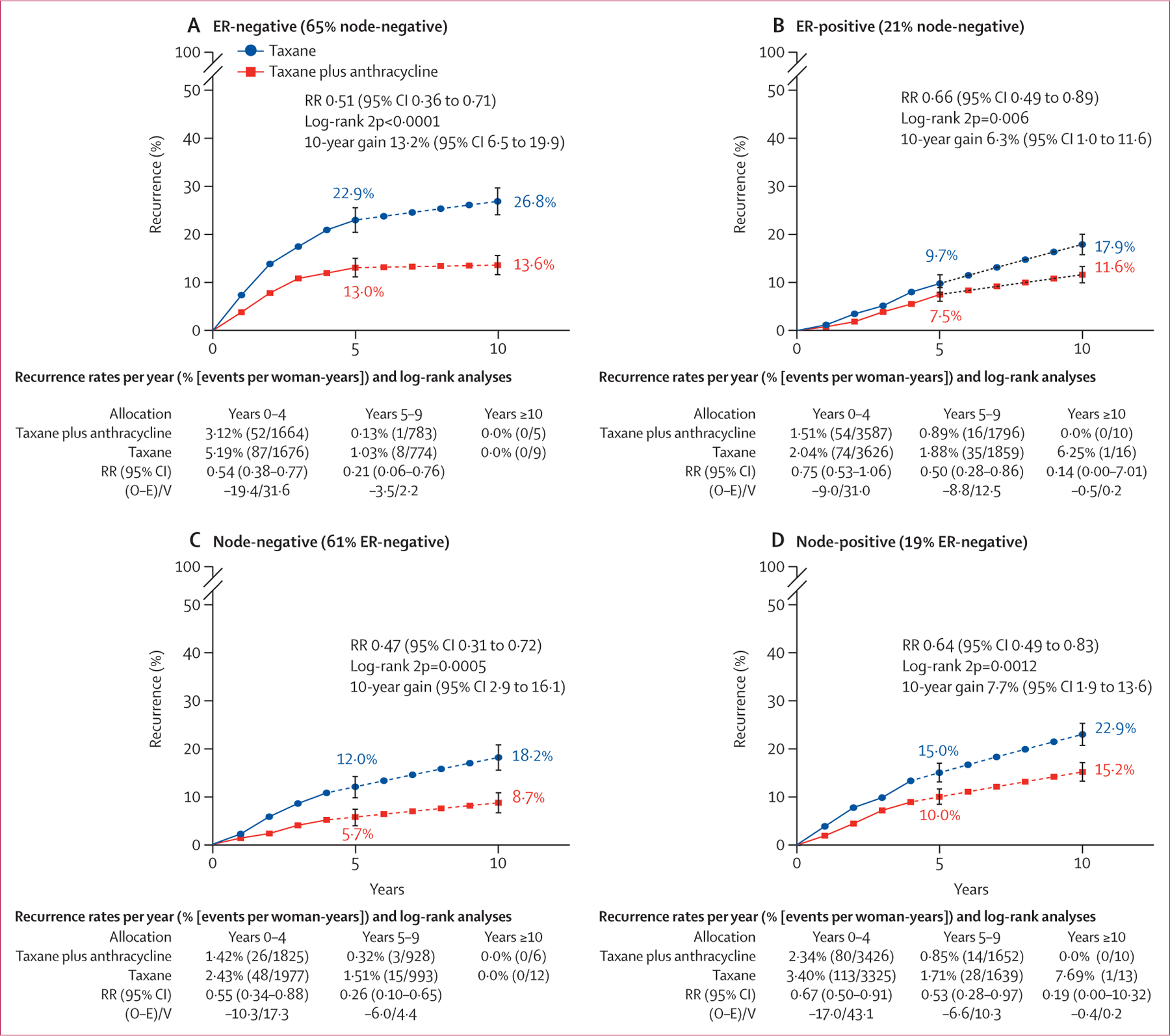
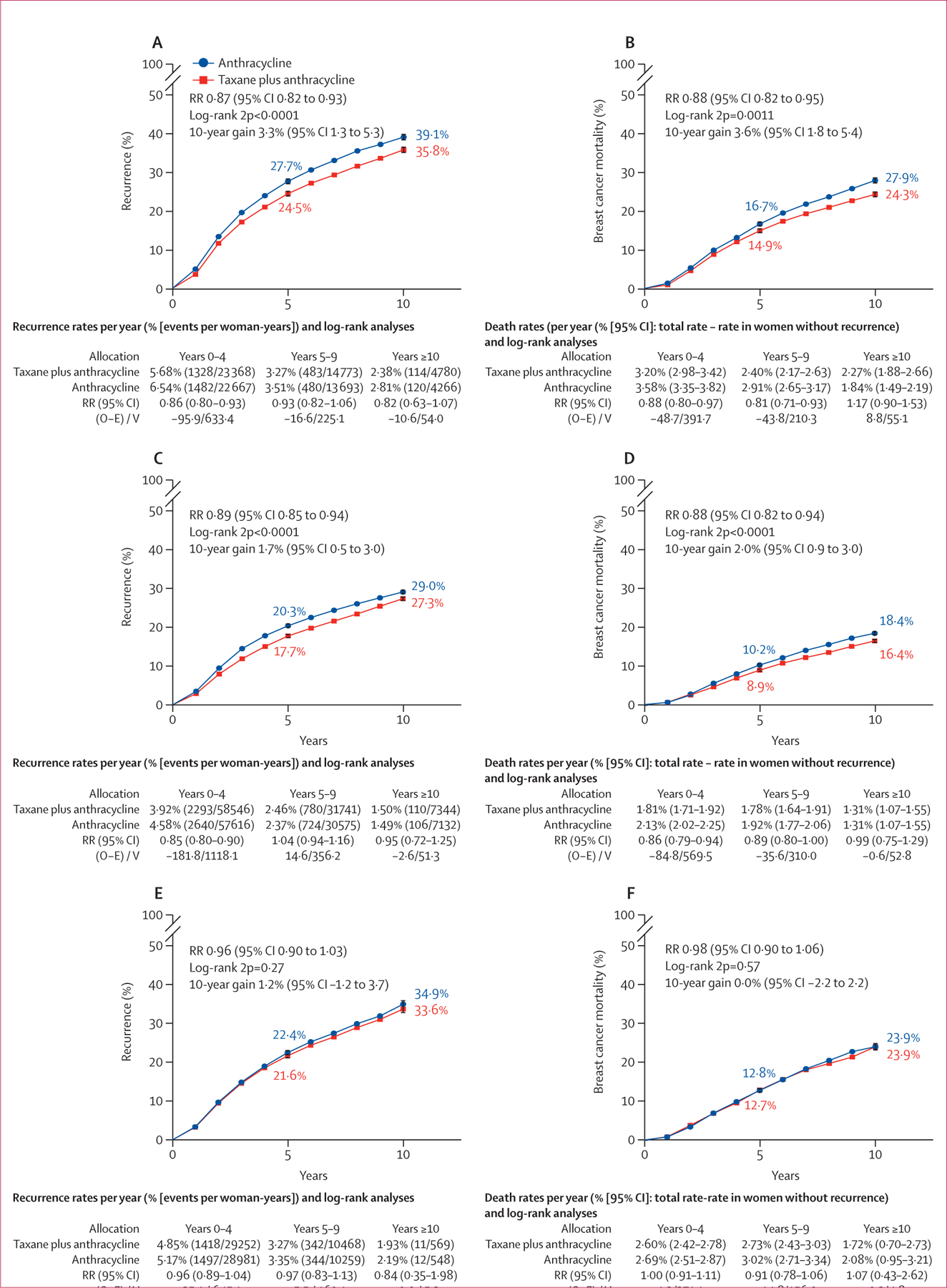
Findings: 28 trials of taxane regimens with or without anthracycline were identified, of which 23 were deemed eligible, and 15 provided data on 18 103 women. Across all 15 trials that provided individual data, recurrence rates were 14% lower on average (RR 0·86, 95% CI 0·79-0·93; p=0·0004) with taxane regimens including anthracycline than those without. Non-breast cancer deaths were not increased but there was one additional acute myeloid leukaemia case per 700 women treated. The clearest reductions in recurrence were found when anthracycline was added concurrently to docetaxel plus cyclophosphamide versus the same dose of docetaxel plus cyclophosphamide (10-year recurrence risk 12·3% vs 21·0%; risk difference 8·7%, 95% CI 4·5-12·9; RR 0·58, 0·47-0·73; p<0·0001). 10-year breast cancer mortality in this group was reduced by 4·2% (0·4-8·1; p=0·0034). No significant reduction in recurrence risk was found for sequential schedules of taxane plus anthracycline when compared with docetaxel plus cyclophosphamide (RR 0·94, 0·83-1·06; p=0·30). For the analysis of anthracycline regimens with versus without taxane, 35 trials (n=52 976) provided individual patient data. Larger recurrence reductions were seen from adding taxane to anthracycline regimens when the cumulative dose of anthracycline was the same in each group (RR 0·87, 0·82-0·93; p<0·0001; n=11 167) than in trials with two-fold higher cumulative doses of non-taxane (mostly anthracycline) in the control group than in the taxane group (RR 0·96, 0·90-1·03; p=0·27; n=14 620). Direct comparisons between anthracycline and taxane regimens showed that a higher cumulative dose and more dose-intense schedules were more efficacious. The proportional reductions in recurrence for taxane plus anthracycline were similar in oestrogen receptor-positive and oestrogen receptor-negative disease, and did not differ by age, nodal status, or tumour size or grade.
Interpretation: Anthracycline plus taxane regimens are most efficacious at reducing breast cancer recurrence and death. Regimens with higher cumulative doses of anthracycline plus taxane provide the greatest benefits, challenging the current trend in clinical practice and guidelines towards non-anthracycline chemotherapy, particularly shorter regimens, such as four cycles of docetaxel-cyclophosphamide. By bringing together data from almost all relevant trials, this meta-analysis provides a reliable evidence base to inform individual treatment decisions, clinical guidelines, and the design of future clinical trials.
Funding: Cancer Research UK, UK Medical Research Council.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests RG reports that EBCTCG is supported by a Cancer Research UK grant paid to the University of Oxford. SA reports institutional grants or contracts from National Institutes of Health/National Cancer Institute, consulting fees from NSBAP Foundation, and participation on a data safety monitoring board or advisory board for Jazz Pharmaceuticals (Study 15-007). JBe reports institutional grants or contracts from Amgen, AstraZeneca, Bayer, Merck, Pfizer, Roche, and Sanofi-Aventis to Karolinska Institute or University Hospital, or both; participation on a data safety monitoring board or advisory board for Stratipath; a leadership or fiduciary role on the Wnt-research; stock or stock options in Stratipath; and honoraria from UpToDate to Asklepios Medicine. JBl reports consulting fees from Myriad Genetics, Seattle Genetics, Immunomedics, Puma Biotechnology, Athenix, OncLive, Biotheranostics, AstraZeneca, Research to Practice, Sanofi, Pfizer, and Tempus; and payments or honoraria for lectures, presentations, speaker's bureaus, and manuscript writing or educational events from Pfizer and Tempus. FC reports consulting fees from Amgen, Astella/Medivation, AstraZeneca, Celgene, Daiichi-Sankyo, Eisai, GE Oncology, Genentech, Gilead, GlaxoSmithKline, Iqvia, Macrogenics, Medscape, Merck-Sharp, Merus BV, Mylan, Mundipharma, Novartis, Pfizer, Pierre-Fabre, priME Oncology, Roche, Sanofi, Samsung Bioepis, Seagen, Teva, and Touchime; participation on a data safety monitoring board or advisory board for Amgen, Astellas/Medivation, AstraZeneca, Celgene, Daiichi-Sankyo, Eisai, GE Oncology, Genentech, Gilead, GlaxoSmithKline, Iqvia, Macrogenics, Medscape, Merck-Sharp, Merus BV, Mylan, Mundipharma, Novartis, Pfizer, Pierre-Fabre, priME Oncology, Roche, Sanofi, Samsung Bioepis, Seagen, Teva, and Touchime; and support for attending meetings or travel (or both) from AstraZeneca, Roche, and Pfizer. JC reports payment or honoraria for lectures, presentations, speaker's bureaus, and manuscript writing or educational events from Pfizer and Pierre Fabre; support for attending meeting or travel (or both) from MSD Oncology, Pfizer, Roche, Daiichi Sankyo Europe, AstraZeneca, and Regeneron; a patent pending for WO2020011770 (A1)—a method of predicting response to treatment in cancer patients; participation on a data safety monitoring board or advisory board for MSD Oncology and AstraZeneca; a leadership or fiduciary role for The Cancer Clinical Research Trust, OncoMark, and OncoAssure; and stock or stock options from OncoMark and OncoAssure. BE reports institutional grants or contracts from AstraZeneca, Eli Lilly, MSD, Novartis, Pfizer, Roche, and Samsung Bioepis, and received support for attending meetings or travel (or both) from MSD. TF reports payments or honoraria for lectures, presentations, speaker's bureaus, and manuscript writing or education events from Lilly and Novartis. NH reports payment or honoraria for lectures, presentations, speaker's bureaus, and manuscript writing or education events from Amgen, AstraZeneca Daiichi-Sankyo, Gilead, Lilly, MSD, Novartis, Pierre-Fabre, Pfizer, Rocher, and Seagen; participation on a data safety monitoring board or advisory board for Gilead, Novartis, Pfizer, Roche, and Seagen; and a leadership or fiduciary role at West German Study Group (WSG). MBJ reports institutional grants or contracts from Samsung Bioepis and Oncology Venture and receives support for attending meetings or travel (or both) from Novartis. EM reports consulting fees from Exact Sciences, Genentech/Roche, Merck, Hologic, Genzyme-Sanofi, and Tersera; payment or honoraria for lectures, presentations, speaker's bureaus, and manuscript writing or educational events from Exact Sciences, Genentech/Roche, and Merck; and stock or stock options from Moderna. LN reports consulting fees from Martell Diagnostic Laboratories, Celgene, Cold Spring Harbour Laboratory, Codagenix, Agenus, Immix Biopharma, QLS Advisors, and Samus Therapeutics. JO reports consulting fees and payment or honoraria for lectures, presentations, speaker's bureaus, and manuscript writing or education events from AbbVie, Agendia, Amgen Biotechnology, Aptitude Health, AstraZeneca, Bayer, Bristol-Myers Squibb, Celgene Corporation, Clovis Oncology, Daiichi Sankyo, Eisai, G1 Therapeutics, Genentech, Gilead Sciences, GRAIL, Halozyme Therapeutics, Heron Therapeutics, Immunomedics, Ipsen Biopharmaceuticals, Lilly, Merck, Myriad, Nektar Therapeutics, Novartis, Pfizer, Pharmacyclics, Pierre Fabre Pharmaceuticals, Puma Biotechnology, Prime Oncology, Roche, Samsung Bioepis, Sanofi, Seagen, Syndax Pharmaceuticals, Taiho Oncology, Tekeda, and Synthon. MP reports institutional grants or contracts from AstraZeneca, Immunomedics, Lilly, Menarini, MSD, Novartis, Pfizer, Radious, Roche–Genentech, Servier, and Synthon; consulting fees from AstraZeneca, Camel-IDS/Precirix, Gilead, Immunomedics, Lilly, Menarini, MSD, Novartis, Pfizer, Roche–Genentech, Seattle Genetics, Immutep, Seagen, NBE Therapeutics, and Frame Therapeutics; and payment or honoraria for lectures, presentations, speaker's bureaus, and manuscript writing or educational events from Roche, Novartis, and MSD. NR reports institutional grants or contracts from Bristol-Myers Squibb. DS reports consulting fees from Eli Lilly and Novartis; a leadership or fiduciary role for BioMarin, TORL BioTherapeutics, and 1200 Pharma; and stock or stock options for Amgen, Seattle Genetics, TORL BioTherapeutics, 1200 Pharma, BioNarin, and Pfizer. SS reports institutional grants or contracts from Genentech/Roche, Kailos Genetics, and BCRF; consulting fees from Roche/Genentech, and Molecular Therapeutics; payment or honoraria for lectures, presentations, speaker's bureaus, and manuscript writing or education events from Genetech/Roche and Daiichi Sankyo; support for attending meetings or travel (or both) from Genentech/Roche, Daiichi Sankyo, and Sanofi; participation on a data safety monitoring board or advisory board for AstraZeneca, Daiichi Sankyo, Exact Sciences, Biotheranostics, Netera, Merck, Silverback Therapeutics, Athenex, Lilly, Aventis, and Inivata; a leadership or fiduciary role for NSABP (Vice Chairman) and CFF (ASCO Director); and third party medical writing for Genentech/Roche and AstraZeneca. GY reports institutional grants or contracts from the US National Cancer Institute to support the NRG Oncology Statistics and Data Management Centre.
Figures
Comment in
-
Benefits and risks of anthracyclines in early-stage breast cancer.Lancet. 2024 Mar 30;403(10433):1239-1240. doi: 10.1016/S0140-6736(23)02889-1. Lancet. 2024. PMID: 38555132 No abstract available.
References
-
- Early Breast Cancer Trialists’ Collaborative Group. Polychemotherapy for early breast cancer: an overview of the randomised trials. Lancet 1998; 352: 930–42. - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005; 365: 1687–717. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
