

Delayed generation of functional virus-specific circulating T follicular helper cells correlates with severe COVID-19
- PMID: 37061513
- PMCID: PMC10105364
- DOI: 10.1038/s41467-023-37835-9
Delayed generation of functional virus-specific circulating T follicular helper cells correlates with severe COVID-19
Abstract
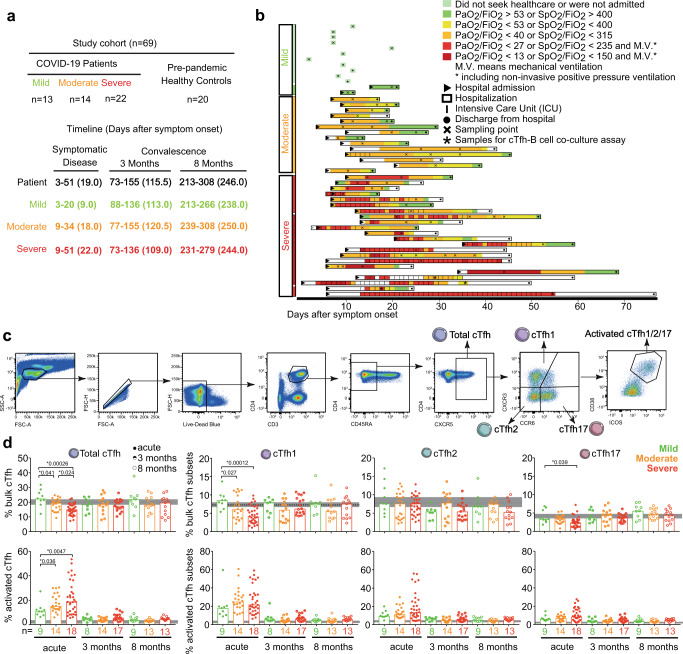
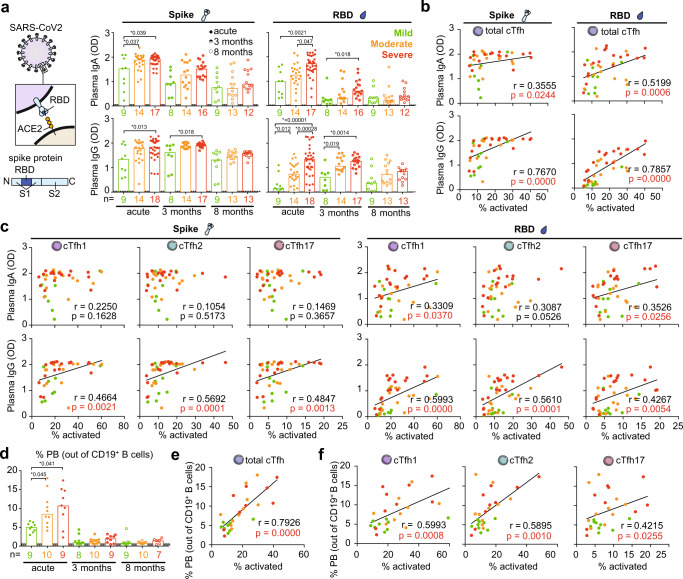
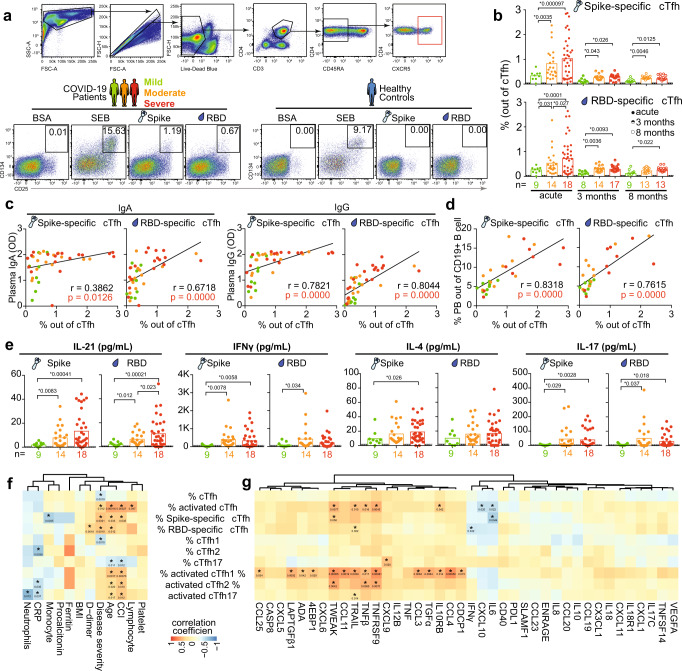
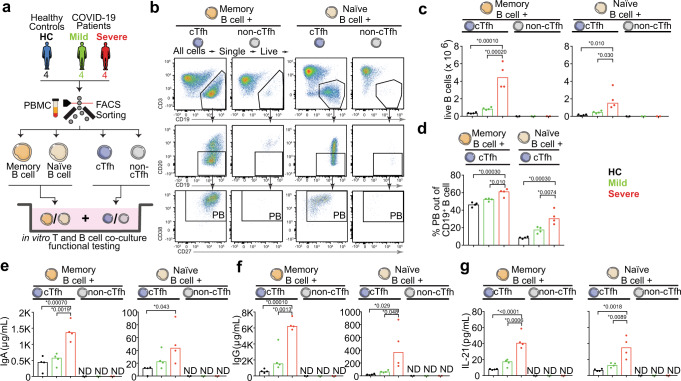
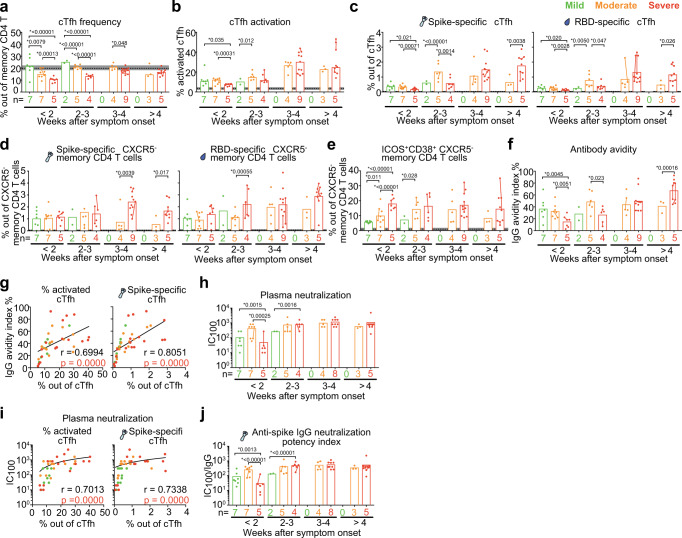
Effective humoral immune responses require well-orchestrated B and T follicular helper (Tfh) cell interactions. Whether these interactions are impaired and associated with COVID-19 disease severity is unclear. Here, longitudinal blood samples across COVID-19 disease severity are analysed. We find that during acute infection SARS-CoV-2-specific circulating Tfh (cTfh) cells expand with disease severity. SARS-CoV-2-specific cTfh cell frequencies correlate with plasmablast frequencies and SARS-CoV-2 antibody titers, avidity and neutralization. Furthermore, cTfh cells but not other memory CD4 T cells, from severe patients better induce plasmablast differentiation and antibody production compared to cTfh cells from mild patients. However, virus-specific cTfh cell development is delayed in patients that display or later develop severe disease compared to those with mild disease, which correlates with delayed induction of high-avidity neutralizing antibodies. Our study suggests that impaired generation of functional virus-specific cTfh cells delays high-quality antibody production at an early stage, potentially enabling progression to severe disease.
© 2023. The Author(s).
Conflict of interest statement
A.S.-S. is a consultant to Astra-Zeneca on studies not related to the present study. The remaining authors declare no competing interests.
Figures
Similar articles
-
SARS-CoV-2-specific circulating T follicular helper cells correlate with neutralizing antibodies and increase during early convalescence.PLoS Pathog. 2021 Jul 16;17(7):e1009761. doi: 10.1371/journal.ppat.1009761. eCollection 2021 Jul. PLoS Pathog. 2021. PMID: 34270631 Free PMC article.
-
T follicular helper cells in the humoral immune response to SARS-CoV-2 infection and vaccination.J Leukoc Biol. 2022 Feb;111(2):355-365. doi: 10.1002/JLB.5MR0821-464R. Epub 2021 Nov 3. J Leukoc Biol. 2022. PMID: 34730247 Free PMC article. Review.
-
T follicular helper cell responses to SARS-CoV-2 vaccination among healthy and immunocompromised adults.Immunol Cell Biol. 2023 Jul;101(6):504-513. doi: 10.1111/imcb.12635. Epub 2023 Mar 23. Immunol Cell Biol. 2023. PMID: 36825370 Free PMC article. Review.
-
Abnormal Shift in B Memory Cell Profile Is Associated With the Expansion of Circulating T Follicular Helper Cells via ICOS Signaling During Acute HIV-1 Infection.Front Immunol. 2022 Feb 10;13:837921. doi: 10.3389/fimmu.2022.837921. eCollection 2022. Front Immunol. 2022. PMID: 35222430 Free PMC article.
-
Circulating follicular helper T cells are increased in systemic sclerosis and promote plasmablast differentiation through the IL-21 pathway which can be inhibited by ruxolitinib.Ann Rheum Dis. 2019 Apr;78(4):539-550. doi: 10.1136/annrheumdis-2018-214382. Epub 2019 Feb 13. Ann Rheum Dis. 2019. PMID: 30760472
Cited by
-
Atypical and non-classical CD45RBlo memory B cells are the majority of circulating SARS-CoV-2 specific B cells following mRNA vaccination or COVID-19.Nat Commun. 2024 Aug 9;15(1):6811. doi: 10.1038/s41467-024-50997-4. Nat Commun. 2024. PMID: 39122676 Free PMC article.
-
Recent Endemic Coronavirus Infection Associates With Higher SARS-CoV-2 Cross-Reactive Fc Receptor Binding Antibodies.bioRxiv [Preprint]. 2024 Oct 23:2024.10.23.619886. doi: 10.1101/2024.10.23.619886. bioRxiv. 2024. Update in: J Virol. 2025 Jun 17;99(6):e0055025. doi: 10.1128/jvi.00550-25. PMID: 39484477 Free PMC article. Updated. Preprint.
-
T cell and autoantibody profiling for primary immune regulatory disorders.medRxiv [Preprint]. 2025 Jan 27:2024.02.25.24303331. doi: 10.1101/2024.02.25.24303331. medRxiv. 2025. Update in: J Allergy Clin Immunol. 2025 Jun 18:S0091-6749(25)00649-9. doi: 10.1016/j.jaci.2025.06.007. PMID: 38464255 Free PMC article. Updated. Preprint.
-
Role of circulating T follicular helper subsets following Ty21a immunization and oral challenge with wild type S. Typhi in humans.Front Immunol. 2024 Sep 12;15:1384642. doi: 10.3389/fimmu.2024.1384642. eCollection 2024. Front Immunol. 2024. PMID: 39328410 Free PMC article.
-
Development of a proteomic signature associated with severe disease for patients with COVID-19 using data from 5 multicenter, randomized, controlled, and prospective studies.Sci Rep. 2023 Nov 20;13(1):20315. doi: 10.1038/s41598-023-46343-1. Sci Rep. 2023. PMID: 37985892 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
