

Real-life experiences with CAR T-cell therapy with idecabtagene vicleucel (ide-cel) for triple-class exposed relapsed/refractory multiple myeloma patients
- PMID: 37061680
- PMCID: PMC10105393
- DOI: 10.1186/s12885-023-10824-3
Real-life experiences with CAR T-cell therapy with idecabtagene vicleucel (ide-cel) for triple-class exposed relapsed/refractory multiple myeloma patients
Abstract
Background: Chimeric antigen receptor (CAR) T-cell therapy has revolutionized the treatment landscape of relapsed/refractory multiple myeloma (RRMM), leading to unprecedented responses in this patient population. Idecabtagene vicleucel (ide-cel) has been recently approved for treatment of triple-class exposed RRMM. We report real-life experiences with the commercial use of ide-cel in RRMM patients.
Methods: We performed a retrospective analysis of the first 16 triple-class exposed RRMM patients treated with ide-cel at a single academic center. We assessed toxicities, response to treatment, CAR T expansion and soluble BCMA (sBCMA) levels.
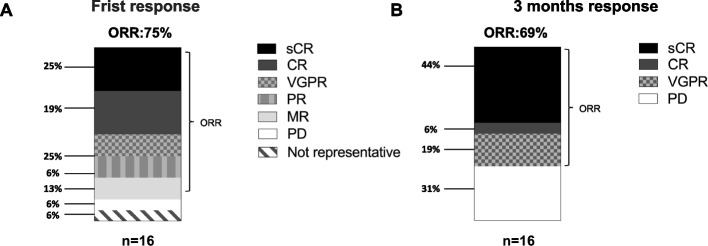
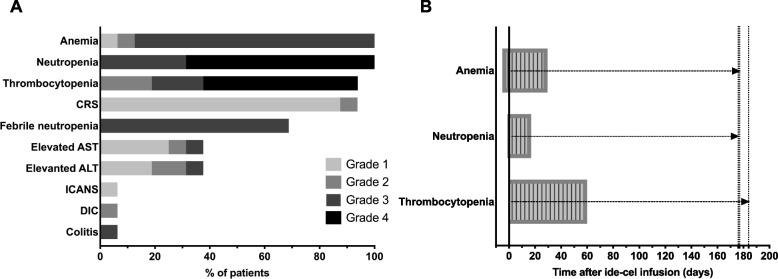
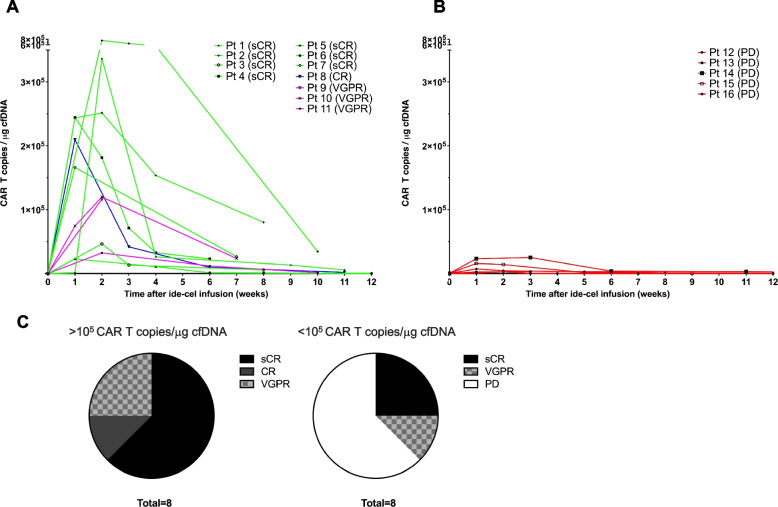
Results: We identified 16 consecutive RRMM patients treated with ide-cel between 06-10/2022. Median age was 69 years, 6 (38%) patients had high-risk cytogenetics, 3 (19%) R-ISS stage III, and 5 (31%) extramedullary disease. Median number of previous treatment lines was 6 (3-12). Manufacturing success rate was 88% (6% required second lymphapheresis, 6% received an out-of-specification product). At 3 months, the overall response rate (ORR) was 69% (44% sCR, 6% CR, 19% VGPR). Cytokine release syndrome (CRS) occurred in 15 (94%) patients (88% G1, 6% G2), immune effector-cell associated neurotoxicity syndrome (ICANS) in 1 (6% G1), febrile neutropenia in 11 (69%), and infections in 5 (31%). Prolonged hematologic toxicity occurred in 4/16 (25%) patients. Other non-hematological toxicities were elevated hepatic enzymes (38%), colitis (6%, G3) and DIC (6%, G2). Responses were more frequent in patients with higher CAR T expansion (100% vs 38%), and lack of decrease or plateau of sBCMA levels was typically observed in non-responders.
Conclusions: We report one of the first cohorts of RRMM treated with commercial ide-cel. The ORR was 69% and safety profile was manageable, but prolonged hematologic toxicity still represents a major challenge. Responses correlated with in vivo CAR T cell expansion, underlining the need of further research to optimize CAR T expansion.
Keywords: CAR-T; Ide-cel; Myeloma; Outcome; Relapsed.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Early Chimeric Antigen Receptor T Cell Expansion Is Associated with Prolonged Progression-Free Survival for Patients with Relapsed/Refractory Multiple Myeloma Treated with Ide-Cel: A Retrospective Monocentric Study.Transplant Cell Ther. 2024 Jun;30(6):630.e1-630.e8. doi: 10.1016/j.jtct.2024.03.003. Epub 2024 Mar 7. Transplant Cell Ther. 2024. PMID: 38458477
-
Idecabtagene vicleucel (ide-cel) CAR T-cell therapy for relapsed and refractory multiple myeloma.Future Oncol. 2022 Jan;18(3):277-289. doi: 10.2217/fon-2021-1090. Epub 2021 Dec 2. Future Oncol. 2022. PMID: 34854741 Review.
-
Phase 2 results of idecabtagene vicleucel (ide-cel, bb2121) in Japanese patients with relapsed and refractory multiple myeloma.Int J Hematol. 2023 May;117(5):729-737. doi: 10.1007/s12185-023-03538-6. Epub 2023 Jan 24. Int J Hematol. 2023. PMID: 36690910 Free PMC article. Clinical Trial.
-
Recent Advances in the Use of Chimeric Antigen Receptor-Expressing T-Cell Therapies for Treatment of Multiple Myeloma.Clin Lymphoma Myeloma Leuk. 2023 Jan;23(1):22-27. doi: 10.1016/j.clml.2022.09.001. Epub 2022 Sep 20. Clin Lymphoma Myeloma Leuk. 2023. PMID: 36411210 Review.
-
Timing of Toxicities and Non-Relapse Mortality Following CAR T Therapy in Myeloma.Transplant Cell Ther. 2024 Sep;30(9):876-884. doi: 10.1016/j.jtct.2024.06.012. Epub 2024 Jun 11. Transplant Cell Ther. 2024. PMID: 38871056
Cited by
-
Novel Immunotherapies and Combinations: The Future Landscape of Multiple Myeloma Treatment.Pharmaceuticals (Basel). 2023 Nov 19;16(11):1628. doi: 10.3390/ph16111628. Pharmaceuticals (Basel). 2023. PMID: 38004493 Free PMC article. Review.
-
An Assessment of the Effectiveness and Safety of Chimeric Antigen Receptor T-Cell Therapy in Multiple Myeloma Patients with Relapsed or Refractory Disease: A Systematic Review and Meta-Analysis.Int J Mol Sci. 2024 May 3;25(9):4996. doi: 10.3390/ijms25094996. Int J Mol Sci. 2024. PMID: 38732213 Free PMC article.
-
Revolutions at the frontline of multiple myeloma treatment: lessons and challenges to finding a cure.Front Oncol. 2025 Jun 20;15:1578529. doi: 10.3389/fonc.2025.1578529. eCollection 2025. Front Oncol. 2025. PMID: 40626006 Free PMC article. Review.
-
Cilta-cel salvages ide-cel failure in relapsed multiple myeloma by driving distinct immune responses.medRxiv [Preprint]. 2025 Jul 11:2025.07.10.25331322. doi: 10.1101/2025.07.10.25331322. medRxiv. 2025. PMID: 40672475 Free PMC article. Preprint.
-
Chimeric Antigen Receptor T Cells in the Treatment of Multiple Myeloma.Hematol Oncol Clin North Am. 2024 Apr;38(2):383-406. doi: 10.1016/j.hoc.2023.12.004. Epub 2023 Dec 28. Hematol Oncol Clin North Am. 2024. PMID: 38158242 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
