

EXCHANGE-2: investigating the efficacy of add-on plasma exchange as an adjunctive strategy against septic shock-a study protocol for a randomized, prospective, multicenter, open-label, controlled, parallel-group trial
- PMID: 37061693
- PMCID: PMC10105400
- DOI: 10.1186/s13063-023-07300-5
EXCHANGE-2: investigating the efficacy of add-on plasma exchange as an adjunctive strategy against septic shock-a study protocol for a randomized, prospective, multicenter, open-label, controlled, parallel-group trial
Abstract
Background: Sepsis is as a life-threatening organ dysfunction caused by a dysregulated host response to an infection. The mortality of sepsis and particular of septic shock is very high. Treatment mostly focuses on infection control but a specific intervention that targets the underlying pathological host response is lacking to the present time. The investigators hypothesize that early therapeutic plasma exchange (TPE) will dampen the maladaptive host response by removing injurious mediators thereby limiting organ dysfunction and improving survival in patients with septic shock. Although small prospective studies demonstrated rapid hemodynamic stabilization under TPE, no adequately powered randomized clinical trial has investigated hard outcomes.
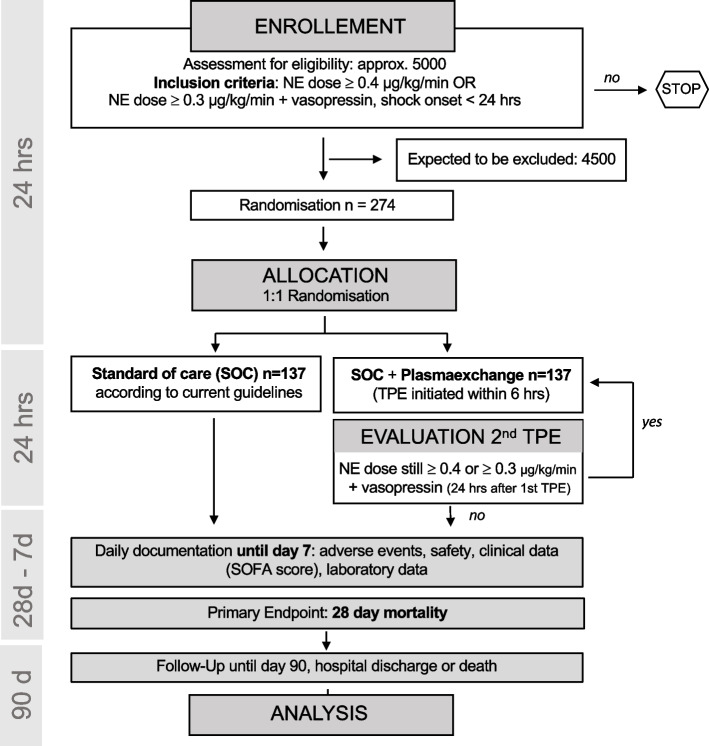
Methods: This is a randomized, prospective, multicenter, open-label, controlled, parallel-group interventional trial to test the adjunctive effect of TPE in patients with early septic shock. Patients with a refractory (defined as norepinephrine (NE) ≥ 0.4 μg/kg/min ≥ 30 min OR NE 0.3 μg/kg/min + vasopressin) and early (shock onset < 24 h) septic shock will be included. The intervention is a standard TPE with donor fresh frozen plasma (1.2 × individual plasma volume) performed within 6 h after randomization and will be compared to a standard of care (SOC) control arm. The primary endpoint is 28 days mortality for which the power analysis revealed a group size of 137 / arm (n = 274) to demonstrate a benefit of 15%. The key secondary objective will be to compare the extent of organ failure indicated by mean SOFA over the first 7 days as well as organ support-free days until day 28 following randomization. Besides numerous biological secondary, safety endpoints such as incidence of bleeding, allergic reactions, transfusion associated lung injury, severe thrombocytopenia, and other severe adverse events will be assessed during the first 7 days. For exploratory scientific analyses, biomaterial will be acquired longitudinally and multiple predefined scientific subprojects are planned. This study is an investigator-initiated trial supported by the German Research Foundation (DFG, DA 1209/7-1), in which 26 different centers in Germany, Switzerland, and Austria will participate over a duration of 33 months.
Discussion: This trial has substantial clinical relevance as it evaluates a promising adjunctive treatment option in refractory septic shock patients suffering from an extraordinary high mortality. A positive trial result could change the current standard of care for this septic subgroup. The results of this study will be disseminated through presentations at international congresses, workshops, and peer-reviewed publications.
Trial registration: ClinicalTrials.gov NCT05726825 , Registered on 14 February 2023.
Keywords: Extracorporeal therapy; Plasmapheresis; Randomized controlled trial; Sepsis; Septic shock.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
