

Genetic testing in children with Brugada syndrome: results from a large prospective registry
- PMID: 37061847
- PMCID: PMC10227762
- DOI: 10.1093/europace/euad079
Genetic testing in children with Brugada syndrome: results from a large prospective registry
Abstract
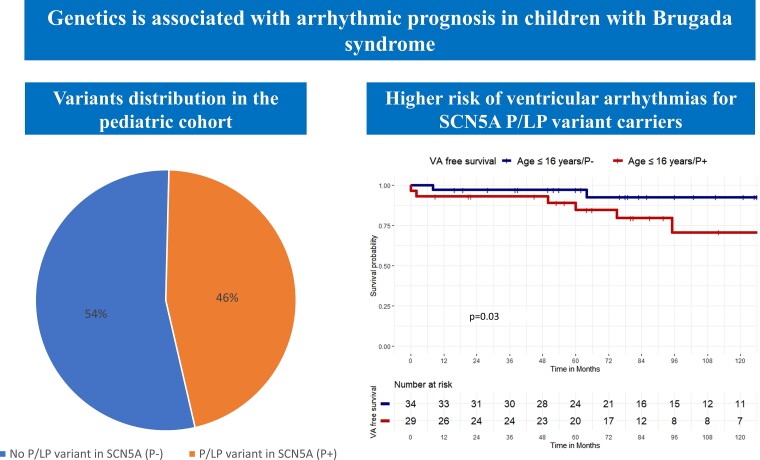
Aims: A pathogenic/likely pathogenic (P/LP) variant in SCN5A is found in 20-25% of patients with Brugada syndrome (BrS). However, the diagnostic yield and prognosis of gene panel testing in paediatric BrS is unclear. The aim of this study is to define the diagnostic yield and outcomes of SCN5A gene testing with ACMG variant classification in paediatric BrS patients compared with adults.
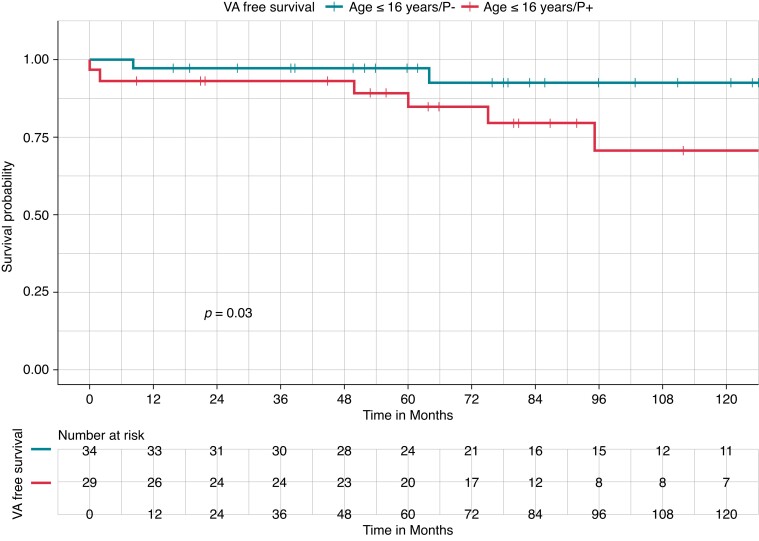
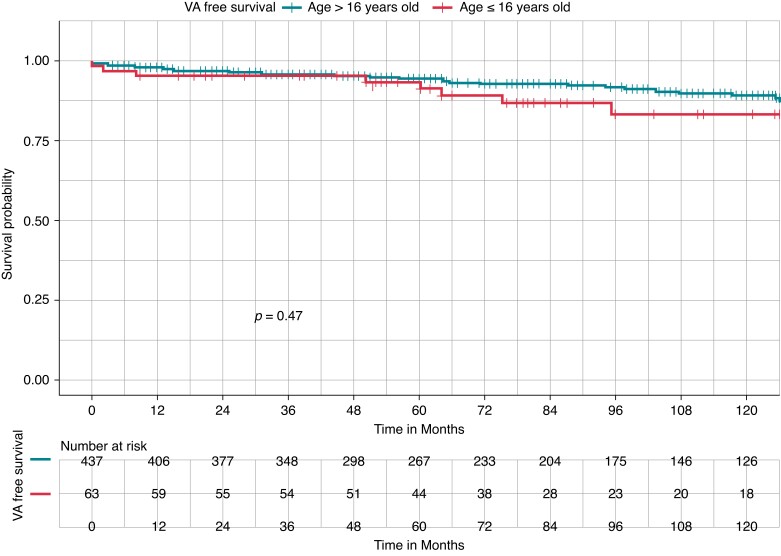
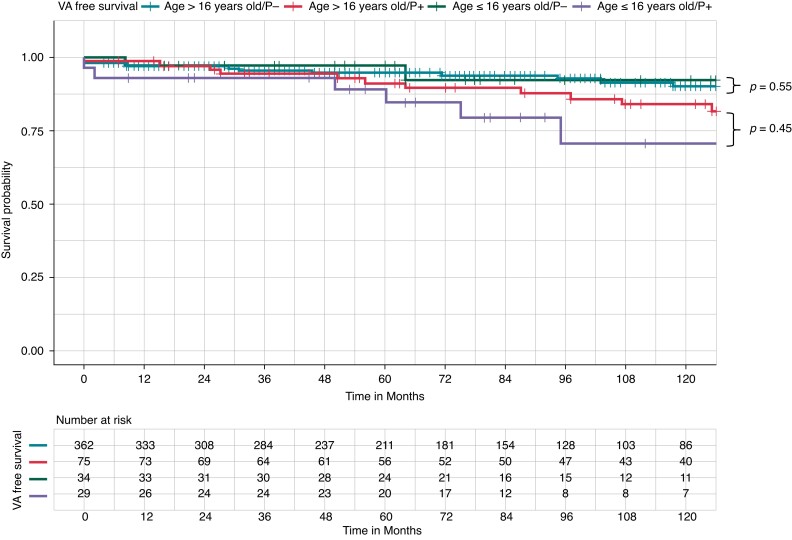
Methods and results: All consecutive patients diagnosed with BrS, between 1992 and 2022, were prospectively enrolled in the UZ Brussel BrS registry. Inclusion criteria were: (i) BrS diagnosis; (ii) genetic analysis performed with a large gene panel; and (iii) classification of gene variants following ACMG guidelines. Paediatric patients were defined as ≤16 years of age. The primary endpoint was ventricular arrhythmias (VAs). A total of 500 BrS patients were included, with 63 paediatric patients and 437 adult patients. Among children with BrS, 29 patients (46%) had a P/LP variant (P+) in SCN5A and no variants were found in 34 (54%) patients (P-). After a mean follow-up of 125.9 months, 8 children (12.7%) experienced a VA, treated with implanted cardioverter defibrillator shock. At survival analysis, P- paediatric patients had higher VA-free survival during the follow-up, compared with P+ paediatric patients. P+ status was an independent predictor of VA. There was no difference in VA-free survival between paediatric and adult BrS patients for both P- and P+.
Conclusion: In a large BrS cohort, the diagnostic yield for P/LP variants in the paediatric population is 46%. P+ children with BrS have a worse arrhythmic prognosis.
Keywords: Brugada syndrome; Genetics; SCN5A; Sudden cardiac death; Ventricular arrhythmias.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: A.B. is a consultant for Biotronik. A.S. received research grants from Daiichi-Sankyo and Bayer; he has received speaker fees from Menarini and Bayer. V.M. received an educational grant from the Foundation ‘Enrico and Enrica Sovena’. M.L.M. is consultant for Atricure. P.B. received compensation for teaching purposes from Biotronik. G.B.C. received compensation for teaching purposes and proctoring from Medtronic, Abbott, Biotronik, Boston Scientific, and Acutus Medical. C.d.A. receives research grants on behalf of the centre from Biotronik, Medtronic, Abbott, LivaNova, Boston Scientific, AtriCure, Philips, and Acutus; C.d.A. received compensation for teaching purposes and proctoring from Medtronic, Abbott, Biotronik, LivaNova, Boston Scientific, Atricure, Acutus Medical Daiichi Sankyo. The remaining authors have nothing to disclose.
Figures
Comment on
-
Characterization and Management of Arrhythmic Events in Young Patients With Brugada Syndrome.J Am Coll Cardiol. 2019 Apr 16;73(14):1756-1765. doi: 10.1016/j.jacc.2019.01.048. J Am Coll Cardiol. 2019. PMID: 30975291
References
-
- Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol 1992;20:1391–6. - PubMed
-
- Priori SG, Wilde AA, Horie M, Cho Y, Behr ER, Berul Cet al. Executive summary: HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. EP Europace 2013;15:1389–1406. - PubMed
-
- Nielsen JC, Lin Y–J, Jansen de Oliveira Figueiredo M, Shamloo AS, Alfie A, Boveda Set al. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) expert consensus on risk assessment in cardiac arrhythmias: use the right tool for the right outcome, in the right population. EP Europace 2020;22:1147–8. - PMC - PubMed
-
- Probst V, Denjoy I, Meregalli PG, Amirault JC, Sacher F, Mansourati Jet al. Clinical aspects and prognosis of Brugada syndrome in children. Circulation 2007;115:2042–8. - PubMed
-
- Michowitz Y, Milman A, Andorin A, Sarquella-Brugada G, Gonzalez Corcia MC, Gourraud JBet al. Characterization and management of arrhythmic events in young patients with Brugada syndrome. J Am Coll Cardiol 2019;73:1756–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
