

A Transcriptome-Based Precision Oncology Platform for Patient-Therapy Alignment in a Diverse Set of Treatment-Resistant Malignancies
- PMID: 37061969
- PMCID: PMC10239356
- DOI: 10.1158/2159-8290.CD-22-1020
A Transcriptome-Based Precision Oncology Platform for Patient-Therapy Alignment in a Diverse Set of Treatment-Resistant Malignancies
Abstract
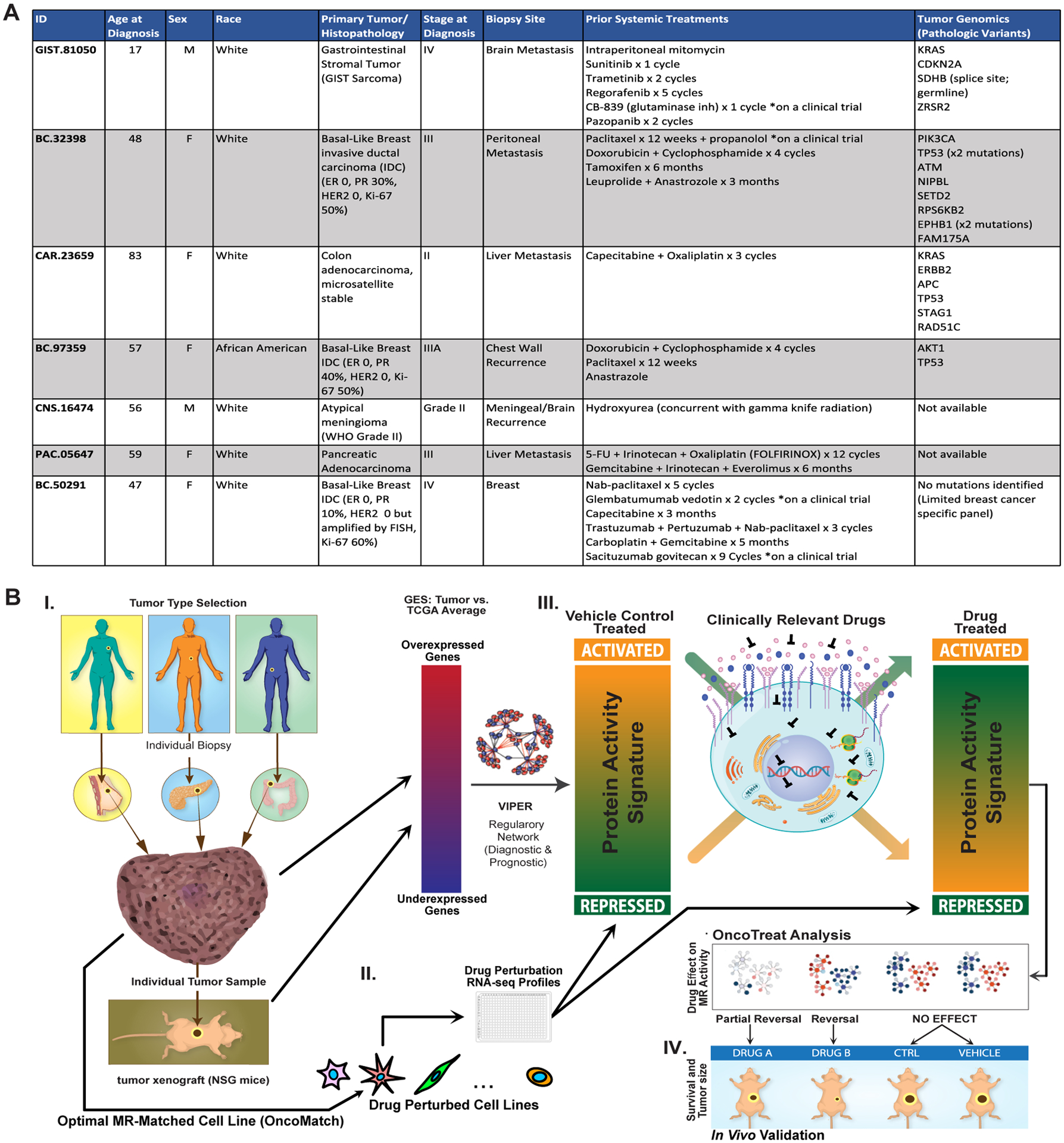
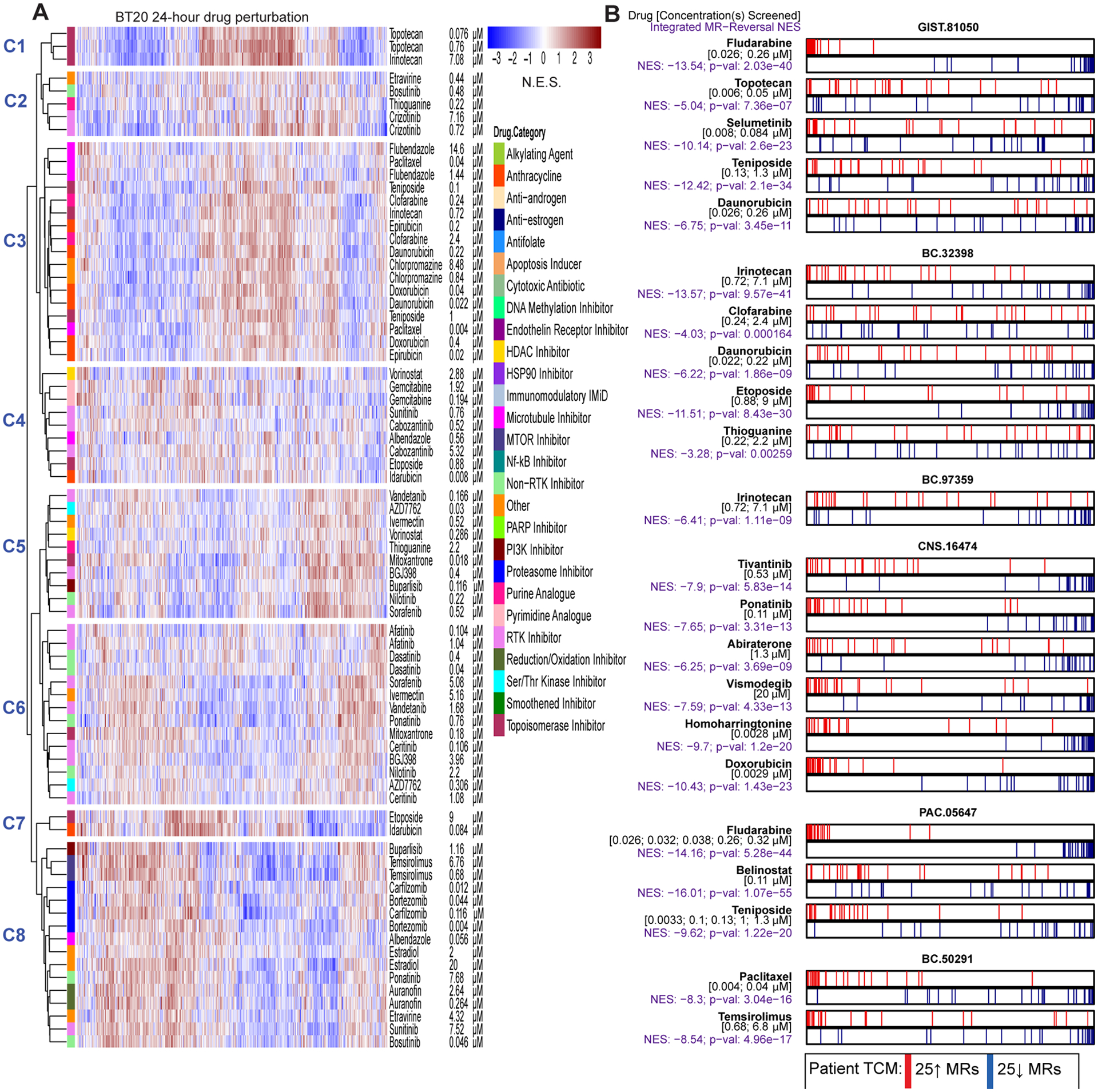
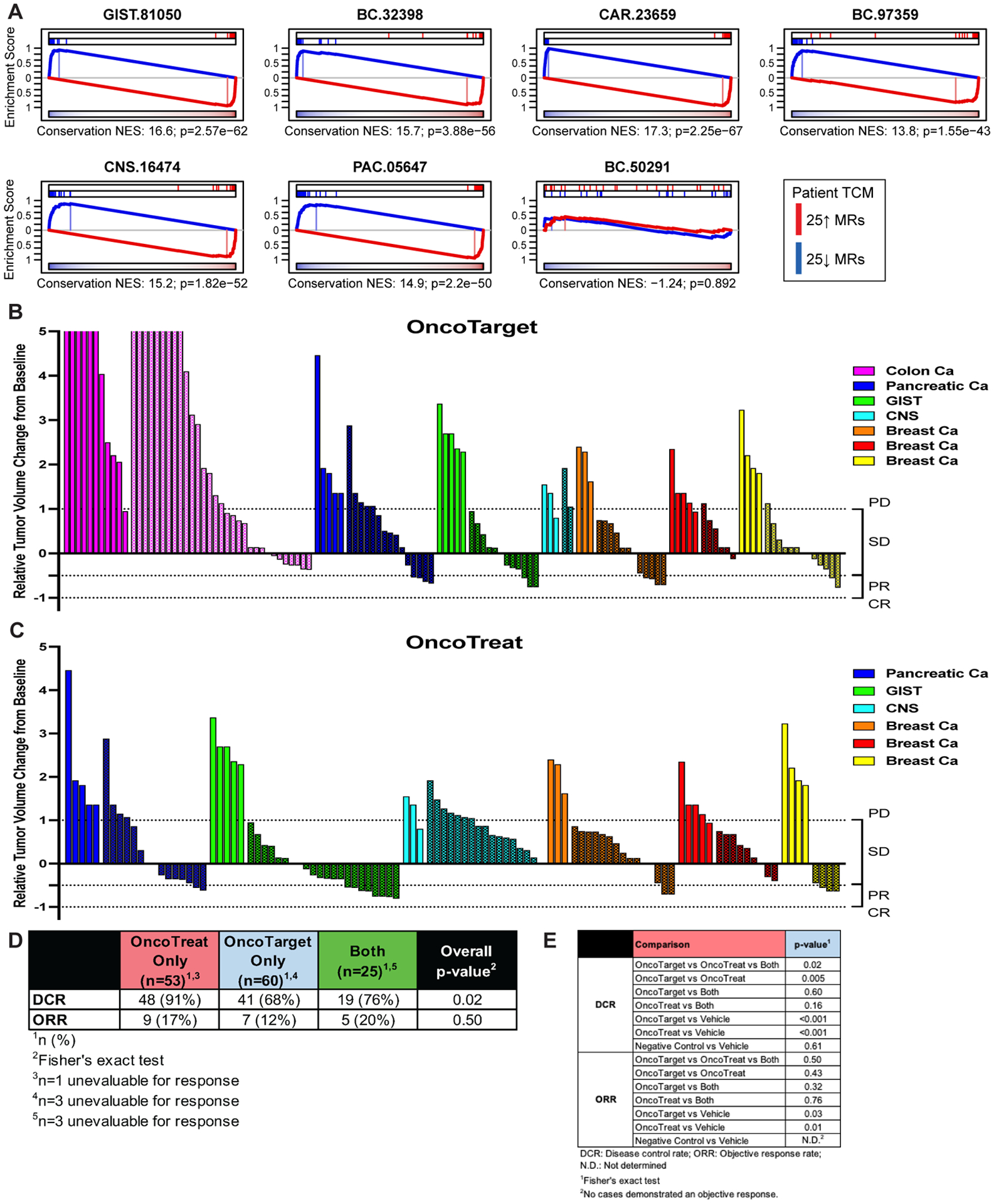
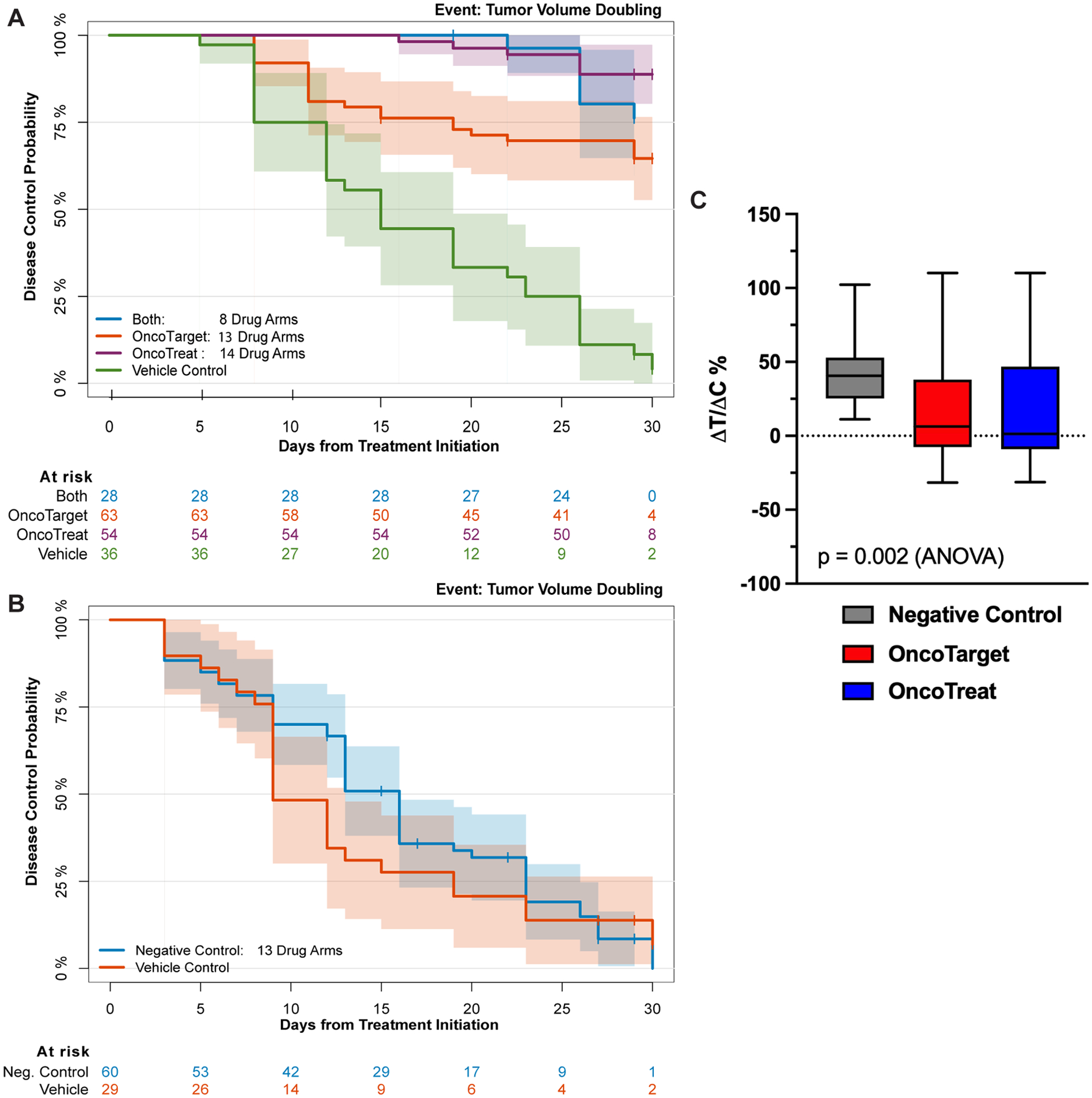
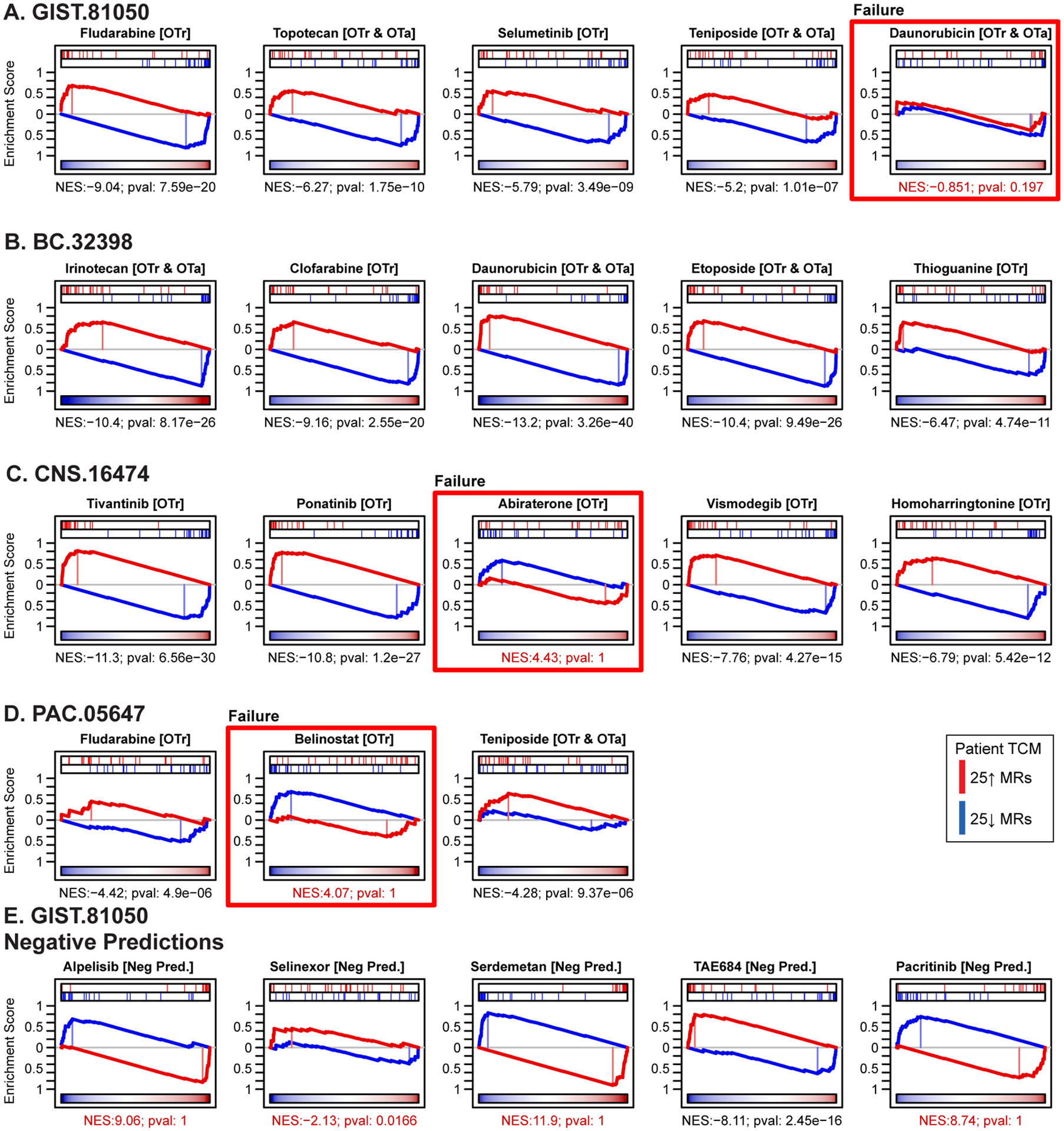
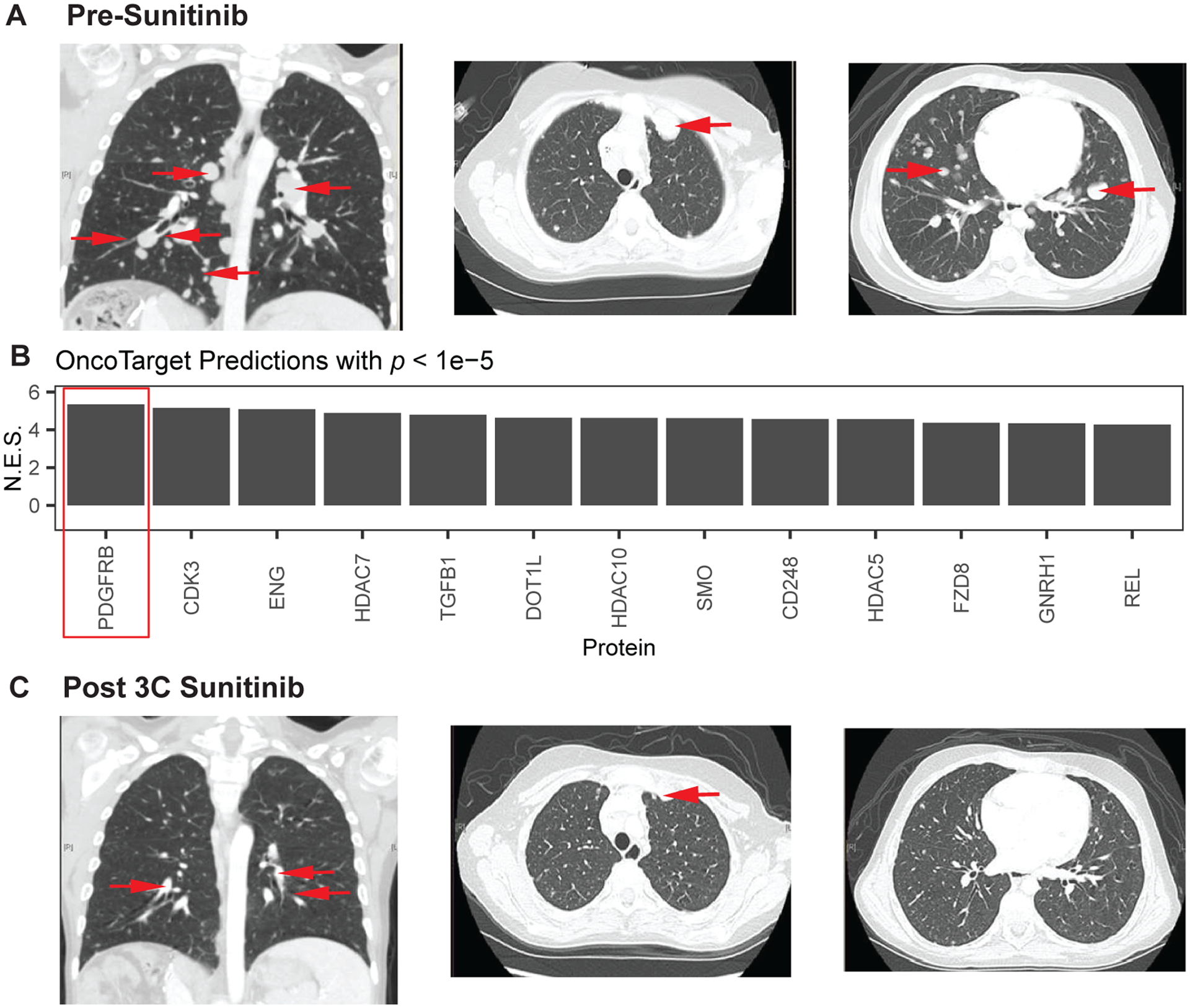
Predicting in vivo response to antineoplastics remains an elusive challenge. We performed a first-of-kind evaluation of two transcriptome-based precision cancer medicine methodologies to predict tumor sensitivity to a comprehensive repertoire of clinically relevant oncology drugs, whose mechanism of action we experimentally assessed in cognate cell lines. We enrolled patients with histologically distinct, poor-prognosis malignancies who had progressed on multiple therapies, and developed low-passage, patient-derived xenograft models that were used to validate 35 patient-specific drug predictions. Both OncoTarget, which identifies high-affinity inhibitors of individual master regulator (MR) proteins, and OncoTreat, which identifies drugs that invert the transcriptional activity of hyperconnected MR modules, produced highly significant 30-day disease control rates (68% and 91%, respectively). Moreover, of 18 OncoTreat-predicted drugs, 15 induced the predicted MR-module activity inversion in vivo. Predicted drugs significantly outperformed antineoplastic drugs selected as unpredicted controls, suggesting these methods may substantively complement existing precision cancer medicine approaches, as also illustrated by a case study.
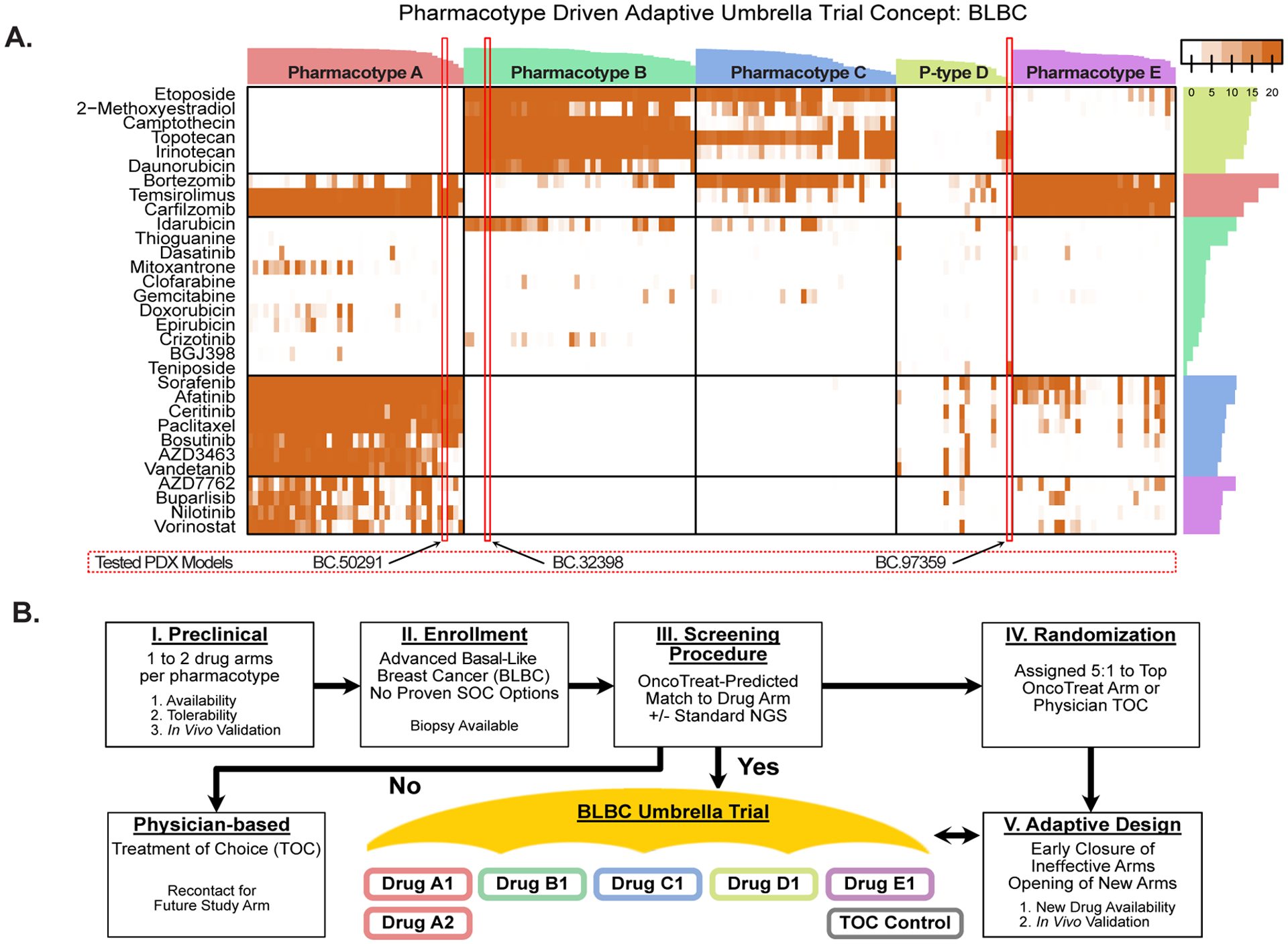
Significance: Complementary precision cancer medicine paradigms are needed to broaden the clinical benefit realized through genetic profiling and immunotherapy. In this first-in-class application, we introduce two transcriptome-based tumor-agnostic systems biology tools to predict drug response in vivo. OncoTarget and OncoTreat are scalable for the design of basket and umbrella clinical trials. This article is highlighted in the In This Issue feature, p. 1275.
©2023 American Association for Cancer Research.
Conflict of interest statement
Conflict of Interest Statement: Dr. Califano is founder, equity holder, and consultant of DarwinHealth Inc., a company that has licensed some of the algorithms used in this manuscript from Columbia University. Dr. Kung is a Medical and Scientific Advisor to DarwinHealth. Columbia University is also an equity holder in DarwinHealth Inc.
Figures
References
-
- Le Tourneau C, Delord JP, Goncalves A, Gavoille C, Dubot C, Isambert N, et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 2015;16(13):1324–34. - PubMed
-
- Tannock IF, Hickman JA. Limits to Personalized Cancer Medicine. N Engl J Med. 2016;375(13):1289–94. - PubMed
-
- Weinstein IB. Cancer. Addiction to oncogenes--the Achilles heal of cancer. Science. 2002;297(5578):63–4. - PubMed
-
- Tang J, Pearce L, O’Donnell-Tormey J, Hubbard-Lucey VM. Trends in the global immuno-oncology landscape. Nat Rev Drug Discov. 2018;17(11):783–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
