

Integrative Analysis of a Large Real-World Cohort of Small Cell Lung Cancer Identifies Distinct Genetic Subtypes and Insights into Histologic Transformation
- PMID: 37062002
- PMCID: PMC10326603
- DOI: 10.1158/2159-8290.CD-22-0620
Integrative Analysis of a Large Real-World Cohort of Small Cell Lung Cancer Identifies Distinct Genetic Subtypes and Insights into Histologic Transformation
Abstract
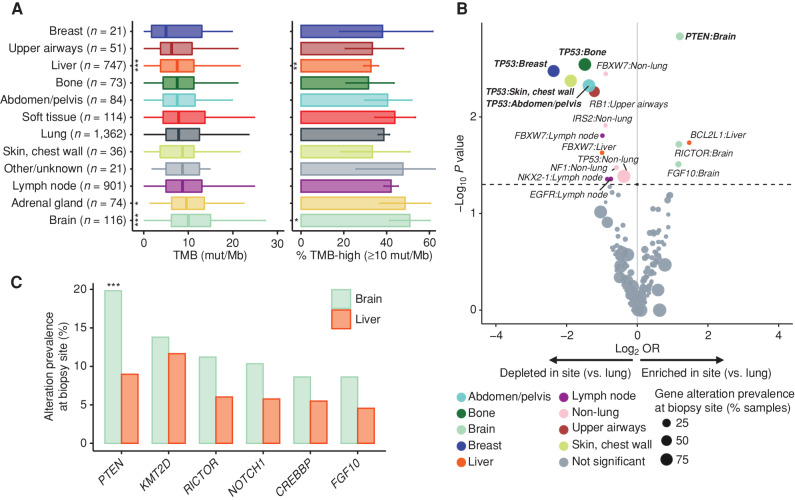
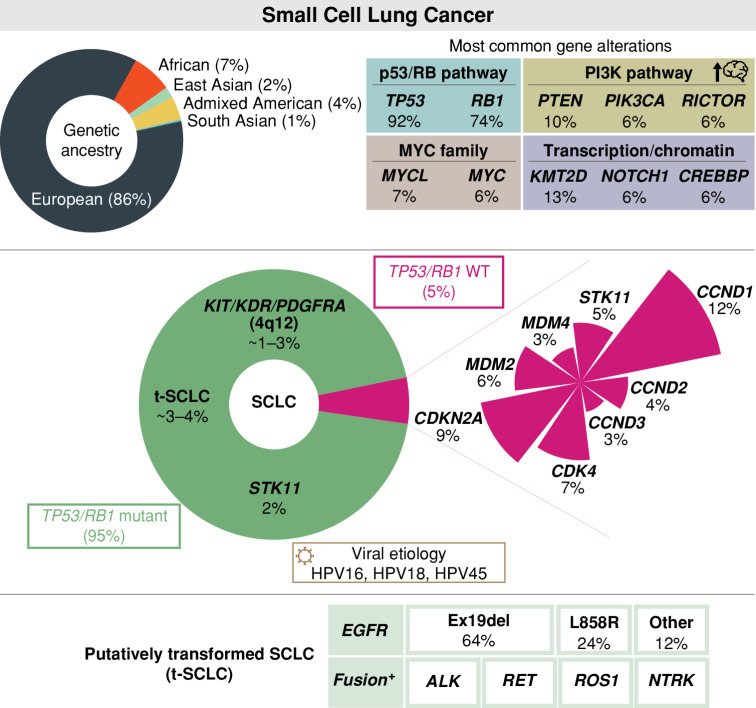
Small cell lung cancer (SCLC) is a recalcitrant neuroendocrine carcinoma with dismal survival outcomes. A major barrier in the field has been the relative paucity of human tumors studied. Here we provide an integrated analysis of 3,600 "real-world" SCLC cases. This large cohort allowed us to identify new recurrent alterations and genetic subtypes, including STK11-mutant tumors (1.7%) and TP53/RB1 wild-type tumors (5.5%), as well as rare cases that were human papillomavirus-positive. In our cohort, gene amplifications on 4q12 are associated with increased overall survival, whereas CCNE1 amplification is associated with decreased overall survival. We also identify more frequent alterations in the PTEN pathway in brain metastases. Finally, profiling cases of SCLC containing oncogenic drivers typically associated with NSCLC demonstrates that SCLC transformation may occur across multiple distinct molecular cohorts of NSCLC. These novel and unsuspected genetic features of SCLC may help personalize treatment approaches for this fatal form of cancer.
Significance: Minimal changes in therapy and survival outcomes have occurred in SCLC for the past four decades. The identification of new genetic subtypes and novel recurrent mutations as well as an improved understanding of the mechanisms of transformation to SCLC from NSCLC may guide the development of personalized therapies for subsets of patients with SCLC. This article is highlighted in the In This Issue feature, p. 1501.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures




Comment in
-
Genetic diversity in small cell lung carcinoma.Transl Lung Cancer Res. 2024 May 31;13(5):1169-1172. doi: 10.21037/tlcr-24-40. Epub 2024 May 17. Transl Lung Cancer Res. 2024. PMID: 38854933 Free PMC article. No abstract available.
References
-
- Horn L, Mansfield AS, Szczesna A, Havel L, Krzakowski M, Hochmair MJ, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med 2018;379:2220–9. - PubMed
-
- Paz-Ares L, Dvorkin M, Chen Y, Reinmuth N, Hotta K, Trukhin D, et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet 2019;394:1929–39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
