

Somatic mosaicism in inborn errors of immunity: Current knowledge, challenges, and future perspectives
- PMID: 37062181
- PMCID: PMC11321052
- DOI: 10.1016/j.smim.2023.101761
Somatic mosaicism in inborn errors of immunity: Current knowledge, challenges, and future perspectives
Abstract
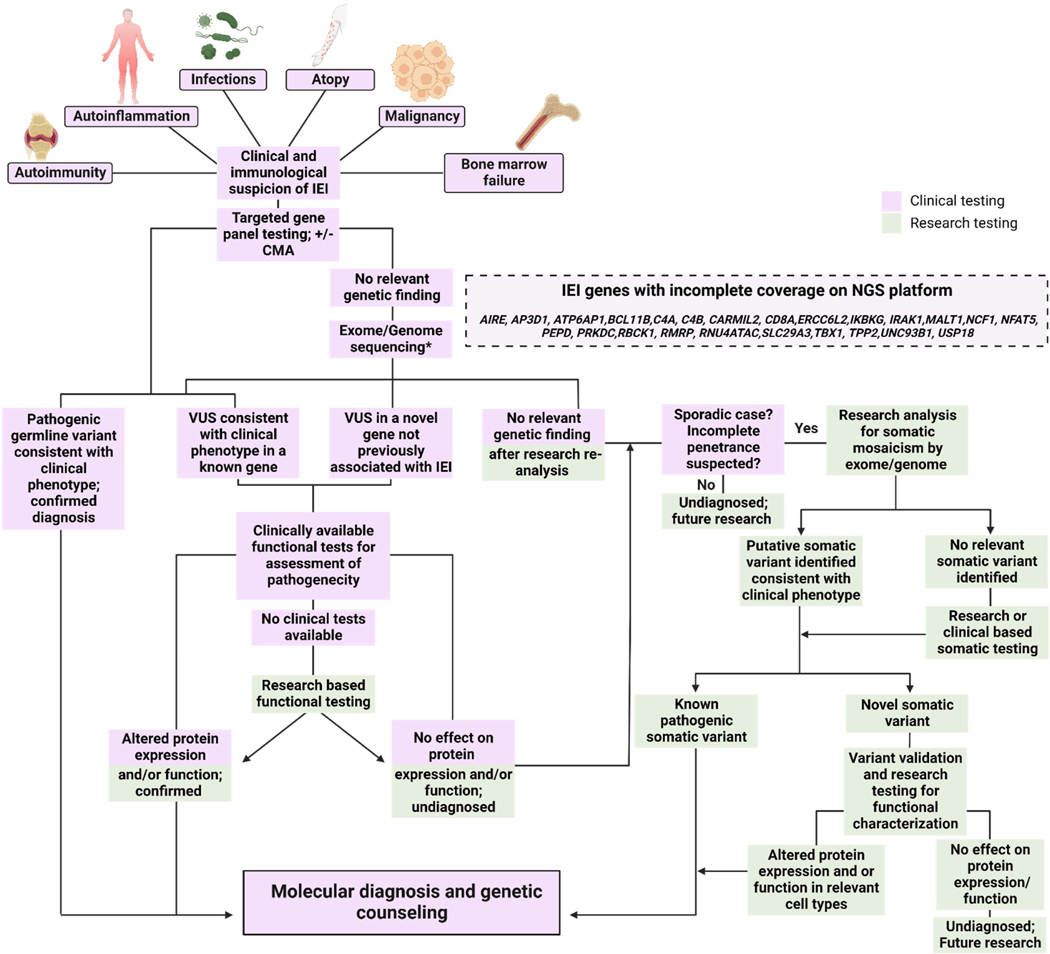
Inborn errors of immunity (IEI) are a diverse group of monogenic disorders of the immune system due to germline variants in genes important for the immune response. Over the past decade there has been increasing recognition that acquired somatic variants present in a subset of cells can also lead to immune disorders or 'phenocopies' of IEI. Discovery of somatic mosaicism causing IEI has largely arisen from investigation of seemingly sporadic cases of IEI with predominant symptoms of autoinflammation and/or autoimmunity in which germline disease-causing variants are not detected. Disease-causing somatic mosaicism has been identified in genes that also cause germline IEI, such as FAS, and in genes without significant corresponding germline disease, such as UBA1 and TLR8. There are challenges in detecting low-level somatic variants, and it is likely that the extent of the somatic mosaicism causing IEI is largely uncharted. Here we review the field of somatic mosaicism leading to IEI and discuss challenges and methods for somatic variant detection, including diagnostic approaches for molecular diagnoses of patients.
Keywords: Genetics; Immunity; Inborn errors of immunity; Mosaicism; Next-generation sequencing; Primary immunodeficiency; Somatic.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare no competing financial interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
