

Efficacy against pneumococcal carriage and the immunogenicity of reduced-dose (0 + 1 and 1 + 1) PCV10 and PCV13 schedules in Ho Chi Minh City, Viet Nam: a parallel, single-blind, randomised controlled trial
- PMID: 37062304
- PMCID: PMC10371874
- DOI: 10.1016/S1473-3099(23)00061-0
Efficacy against pneumococcal carriage and the immunogenicity of reduced-dose (0 + 1 and 1 + 1) PCV10 and PCV13 schedules in Ho Chi Minh City, Viet Nam: a parallel, single-blind, randomised controlled trial
Abstract
Background: Interest in reduced-dose pneumococcal conjugate vaccine (PCV) schedules is growing, but data on their ability to provide direct and indirect protection are scarce. We evaluated 1 + 1 (at 2 months and 12 months) and 0 + 1 (at 12 months) schedules of PCV10 or PCV13 in a predominately unvaccinated population.
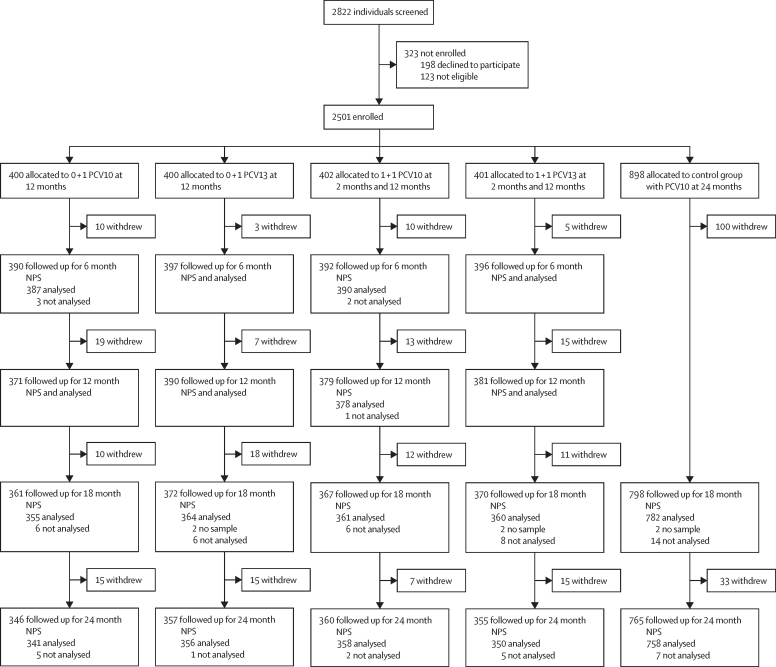
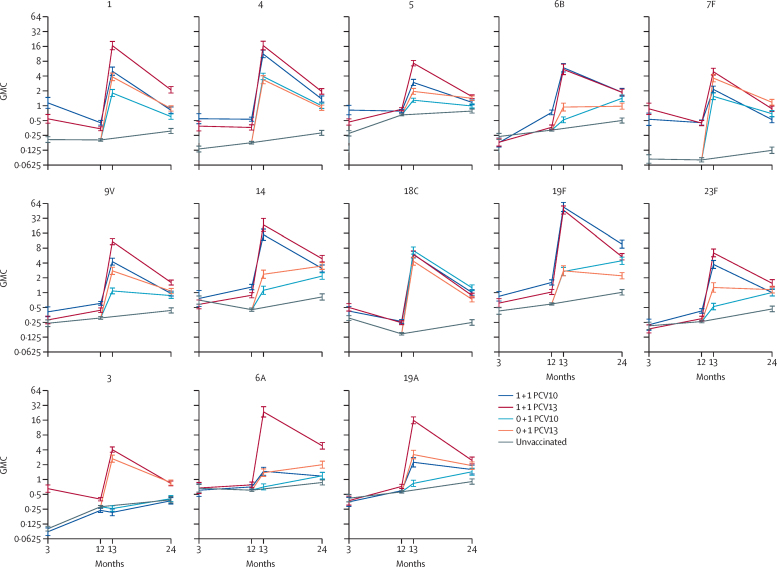
Methods: In this parallel, single-blind, randomised controlled trial, healthy infants aged 2 months were recruited from birth records in three districts in Ho Chi Minh City, Vietnam, and assigned (4:4:4:4:9) to one of five groups: PCV10 at 12 months of age (0 + 1 PCV10), PCV13 at 12 months of age (0 + 1 PCV13), PCV10 at 2 months and 12 months of age (1 + 1 PCV10), PCV13 at 2 months and 12 months of age (1 + 1 PCV13), and unvaccinated control. Outcome assessors were masked to group allocation, and the infants' caregivers and those administering vaccines were not. Nasopharyngeal swabs collected at 6 months, 12 months, 18 months, and 24 months were analysed for pneumococcal carriage. Blood samples collected from a subset of participants (200 per group) at various timepoints were analysed by ELISA and opsonophagocytic assay. The primary outcome was the efficacy of each schedule against vaccine-type carriage at 24 months, analysed by intention to treat for all those with a nasopharyngeal swab available. This trial is registered at ClinicalTrials.gov, NCT03098628.
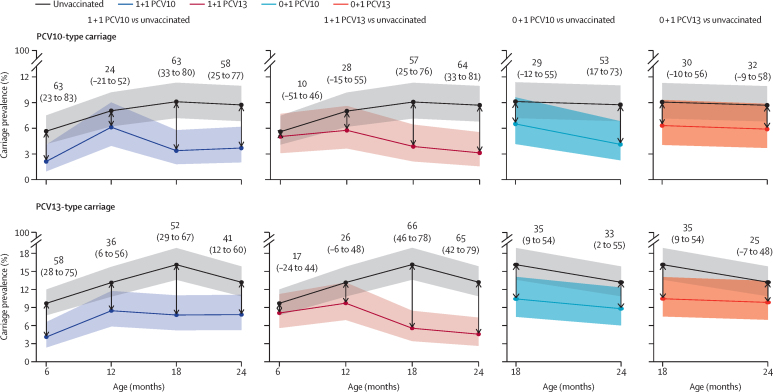
Findings: 2501 infants were enrolled between March 8, 2017, and July 24, 2018 and randomly assigned to study groups (400 to 0 + 1 PCV10, 400 to 0 + 1 PCV13, 402 to 1 + 1 PCV10, 401 to 1 + 1 PCV13, and 898 to control). Analysis of the primary endpoint included 341 participants for 0 + 1 PCV10, 356 0 + 1 PCV13, 358 1 + 1 PCV10, 350 1 + 1 PCV13, and 758 control. At 24 months, a 1 + 1 PCV10 schedule reduced PCV10-type carriage by 58% (95% CI 25 to 77), a 1 + 1 PCV13 schedule reduced PCV13-type carriage by 65% (42 to 79), a 0 + 1 PCV10 schedule reduced PCV10-type carriage by 53% (17 to 73), and a 0 + 1 PCV13 schedule non-significantly reduced PCV13-type carriage by 25% (-7 to 48) compared with the unvaccinated control group. Reactogenicity and serious adverse events were similar across groups.
Interpretation: A 1 + 1 PCV schedule greatly reduces vaccine-type carriage and is likely to generate substantial herd protection and provide some degree of individual protection during the first year of life. Such a schedule is suitable for mature PCV programmes or for introduction in conjunction with a comprehensive catch-up campaign, and potentially could be most effective given as a mixed regimen (PCV10 then PCV13). A 0 + 1 PCV schedule has some effect on carriage along with a reasonable immune response and could be considered for use in humanitarian crises or remote settings.
Funding: Bill & Melinda Gates Foundation.
Translation: For the Vietnamese translation of the abstract see Supplementary Materials section.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests All authors received salary support from the Bill & Melinda Gates Foundation grant. KM and CS are investigators on a clinical research collaboration with Pfizer on PCV vaccination in Mongolia and are investigators on a Merck Investigator Studies Program grant funded by MSD on pneumococcal serotype epidemiology in children.
Figures
Comment in
-
1 + 1 dose schedule for pneumococcal child vaccination: new normal?Lancet Infect Dis. 2023 Aug;23(8):884-885. doi: 10.1016/S1473-3099(23)00065-8. Epub 2023 Apr 14. Lancet Infect Dis. 2023. PMID: 37062299 No abstract available.
Similar articles
-
Immunogenicity and reactogenicity of ten-valent versus 13-valent pneumococcal conjugate vaccines among infants in Ho Chi Minh City, Vietnam: a randomised controlled trial.Lancet Infect Dis. 2019 May;19(5):497-509. doi: 10.1016/S1473-3099(18)30734-5. Epub 2019 Apr 8. Lancet Infect Dis. 2019. PMID: 30975525 Free PMC article. Clinical Trial.
-
Immunogenicity of alternative ten-valent pneumococcal conjugate vaccine schedules in infants in Ho Chi Minh City, Vietnam: results from a single-blind, parallel-group, open-label, randomised, controlled trial.Lancet Infect Dis. 2021 Oct;21(10):1415-1428. doi: 10.1016/S1473-3099(20)30775-1. Epub 2021 Jun 23. Lancet Infect Dis. 2021. PMID: 34171233 Free PMC article. Clinical Trial.
-
Effect of a 2+1 schedule of ten-valent versus 13-valent pneumococcal conjugate vaccine on pneumococcal carriage: Results from a randomised controlled trial in Vietnam.Vaccine. 2021 Apr 15;39(16):2303-2310. doi: 10.1016/j.vaccine.2021.02.043. Epub 2021 Mar 19. Vaccine. 2021. PMID: 33745731 Free PMC article. Clinical Trial.
-
The impact of pneumococcal conjugate vaccines on serotype 19A nasopharyngeal carriage.Expert Rev Vaccines. 2019 Dec;18(12):1243-1270. doi: 10.1080/14760584.2019.1675521. Expert Rev Vaccines. 2019. PMID: 31587592
-
Effects of PCV10 and PCV13 on pneumococcal serotype 6C disease, carriage, and antimicrobial resistance.Vaccine. 2024 Apr 30;42(12):2983-2993. doi: 10.1016/j.vaccine.2024.03.065. Epub 2024 Mar 28. Vaccine. 2024. PMID: 38553292
Cited by
-
Bifidobacteria support optimal infant vaccine responses.Nature. 2025 May;641(8062):456-464. doi: 10.1038/s41586-025-08796-4. Epub 2025 Apr 2. Nature. 2025. PMID: 40175554 Free PMC article.
-
Effect of a Reduced PCV10 Dose Schedule on Pneumococcal Carriage in Vietnam.N Engl J Med. 2024 Nov 28;391(21):1992-2002. doi: 10.1056/NEJMoa2400007. N Engl J Med. 2024. PMID: 39602629 Free PMC article. Clinical Trial.
-
Prevalence of nasopharyngeal Streptococcus Pneumoniae carriage in infants: A systematic review and meta-analysis of cohort studies and randomized controlled trials.PLoS One. 2024 Dec 18;19(12):e0315461. doi: 10.1371/journal.pone.0315461. eCollection 2024. PLoS One. 2024. PMID: 39693316 Free PMC article.
-
The microbiological characteristics and diagnosis of Streptococcus pneumoniae infection in the conjugate vaccine era.Hum Vaccin Immunother. 2025 Dec;21(1):2497611. doi: 10.1080/21645515.2025.2497611. Epub 2025 Apr 27. Hum Vaccin Immunother. 2025. PMID: 40289536 Free PMC article. Review.
-
Inequitable Distribution of Global Economic Benefits from Pneumococcal Conjugate Vaccination.Vaccines (Basel). 2024 Jul 12;12(7):767. doi: 10.3390/vaccines12070767. Vaccines (Basel). 2024. PMID: 39066405 Free PMC article.
References
-
- Davis SM, Deloria-Knoll M, Kassa HT, O'Brien KL. Impact of pneumococcal conjugate vaccines on nasopharyngeal carriage and invasive disease among unvaccinated people: review of evidence on indirect effects. Vaccine. 2013;32:133–145. - PubMed
-
- WHO Pneumococcal conjugate vaccines in infants and children under 5 years of age: WHO position paper—February 2019. Wkly Epidemiol Rec. 2019;94:85–104.
-
- O'Brien KL. When less is more: how many doses of PCV are enough? Lancet Infect Dis. 2018;18:127–128. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
