

Mechanical mapping of the prostate in vivo using Dynamic Instrumented Palpation; towards an in vivo strategy for cancer assessment
- PMID: 37062899
- PMCID: PMC10251469
- DOI: 10.1177/09544119231154305
Mechanical mapping of the prostate in vivo using Dynamic Instrumented Palpation; towards an in vivo strategy for cancer assessment
Abstract
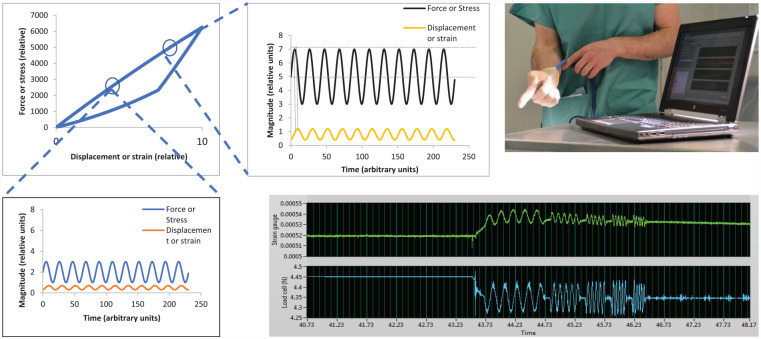
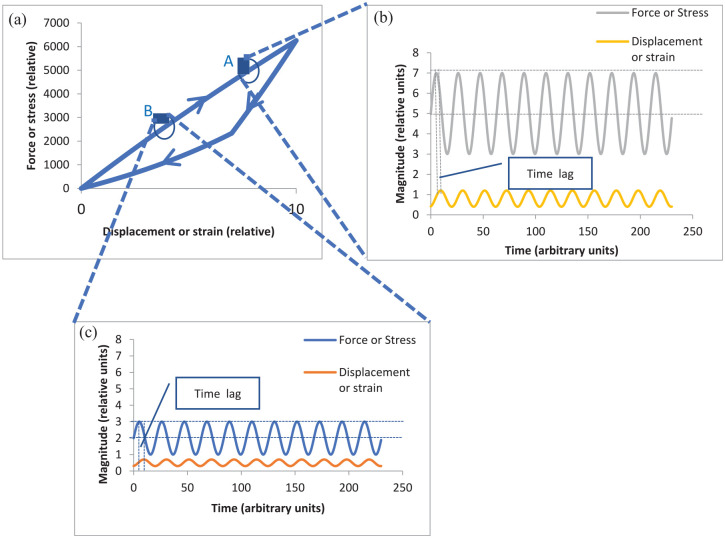
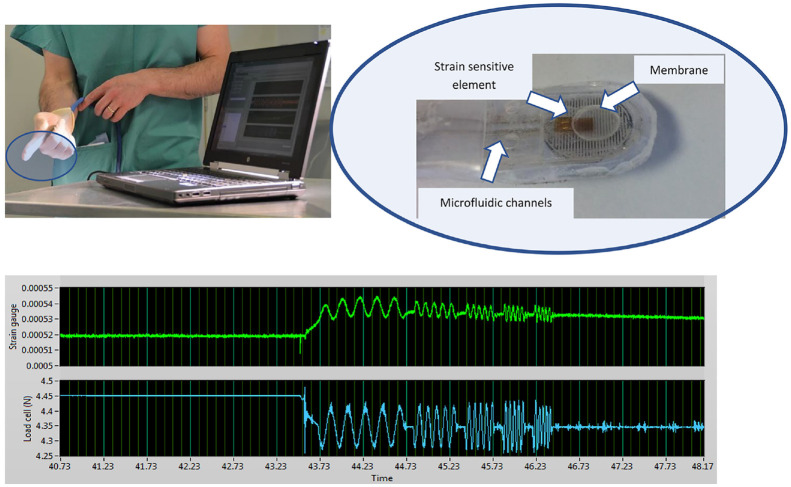
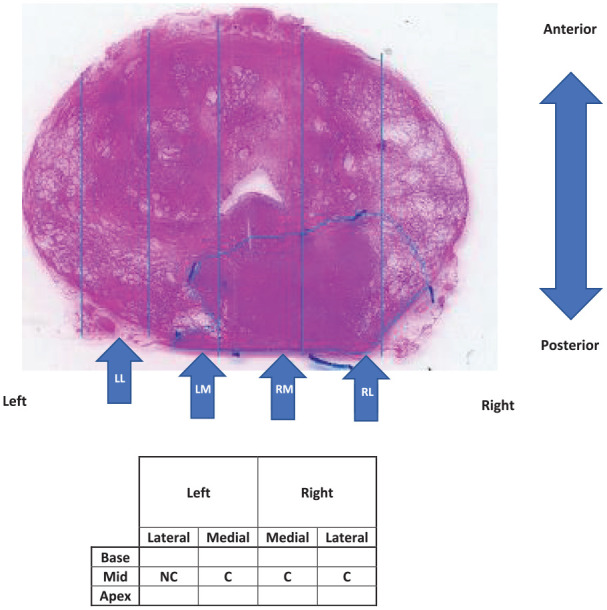
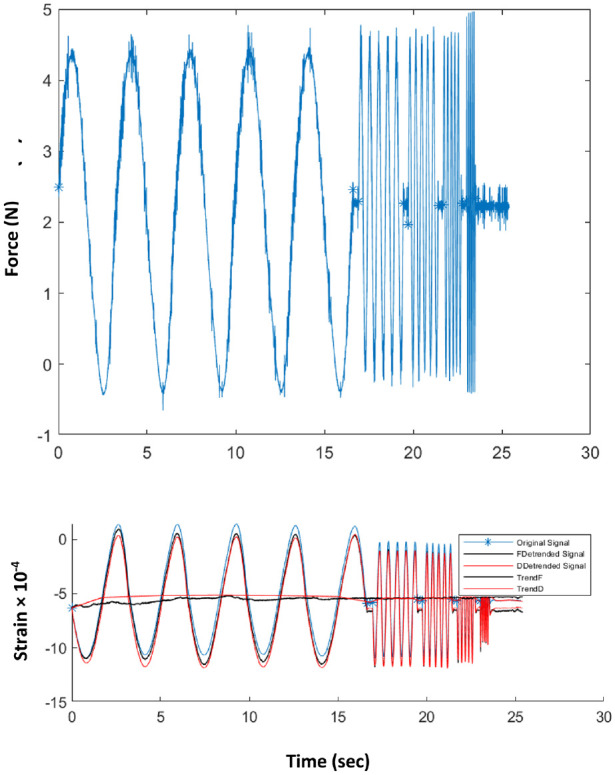
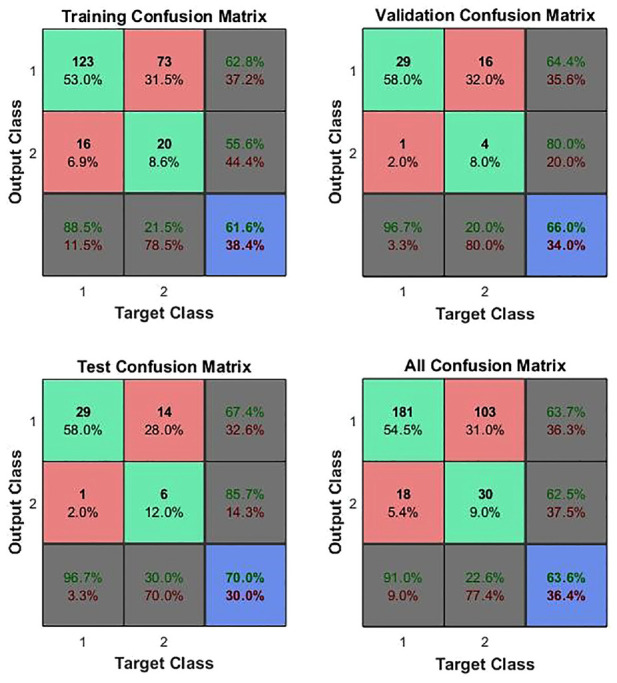
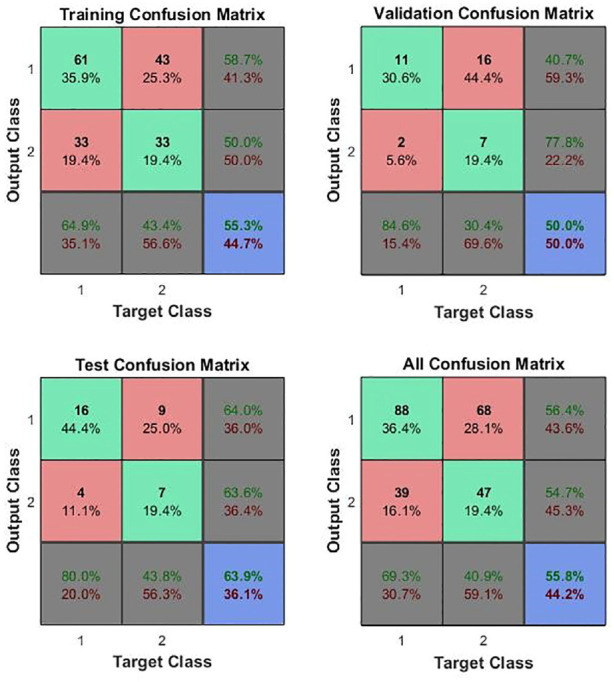
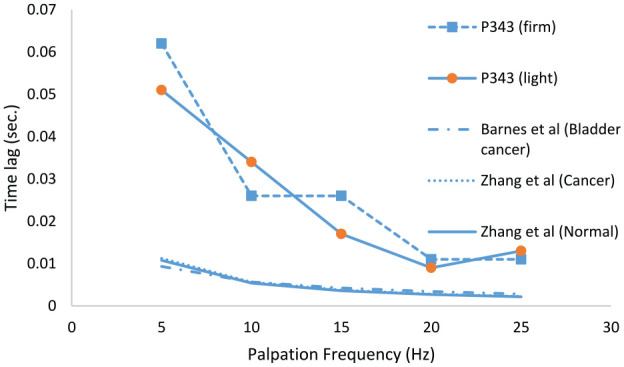
A calibrated palpation sensor has been developed for making instrumented Digital Rectal Examinations (iDREs) with a view to assessing patients for prostate cancer. The instrument measures the dynamic stiffness of the palpable surface of the prostate, and has been trialled on 12 patients in vivo. The patients had been diagnosed with prostate cancer and were scheduled for radical prostatectomy. As far as possible, patients with asymmetric disease were chosen so as to give a variation in gland condition over the palpable surface. The device works by applying an oscillating pressure (force) to a flexible probe whose displacement into the tissue is also measured in order to yield a dynamic stiffness, the static stiffness being incidentally measured at the mean oscillatory force. The device was deployed mounted on the index finger of a urologist and measurements taken at 12-16 positions on each patient using light and firm pressure and palpation frequencies of 1 or 5 Hz. In parallel, conventional DRE assessments were made by a consultant urologist for cancer. After in vivo measurement, the glands were removed and examined histologically with each palpation point being classified as cancerous (C) or not (NC). The work has established the first measurements of static modulus of living prostate tissue to be: 26.8 (13.3) kPa for tissue affected by prostate cancer (C classification), and 24.8 kPa (11.9) for tissue unaffected by cancer (NC classification), values quoted as median (interquartile range). The dynamic properties were characterised by: dynamic modulus, 5.15 kPa (4.86) for the C classification and 4.61 kPa (3.08) for the NC classification and the time lag between force and displacement at 5 Hz palpation frequency, 0.0175 s (0.0078) for the C classification and 0.0186 s (0.0397) for the NC classification, values again quoted as median (interquartile range). With the limited set of features that could be generated, an Artificial Neural Network (ANN) classification yielded a sensitivity of 97%, negative predictive value of 86%, positive predictive value of 67% and accuracy of 70% but with relatively poor specificity (30%). Besides extending the feature set, there are a number of changes in probe design, probing strategy and in mechanics analysis, which are expected to improve the diagnostic capabilities of the method.
Keywords: Prostate cancer diagnosis; dynamic stiffness; elastic modulus; in vivo; relaxation time.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors RLR, AMcN and OJ have plans to develop and market a device based on the technology presented here, US patent no. 15/898,768.
Figures
References
-
- Burford DC, Austoker KM. Prostate cancer risk management programme information for primary care; PSA testing in asymptomatic men., Evidence Document: NHS Cancer Screening Programmes, 2010.
-
- Gleason DF. Histologic grading of prostate cancer: A perspective. Hum Pathol 1992; 23(3): 273–279. - PubMed
-
- Epstein JI. An update of the Gleason grading system. J Urol 2010; 183(2): 433–440. - PubMed
-
- Carvalhal GF, Smith DS, Mager DE, et al. Digital rectal examination for detecting prostate cancer at prostate specific antigen levels of 4ng/ml or less. J. Urol 2010; 161(3): 835–839. - PubMed
-
- Rosenkrantz AB, Kim S, Lim RP, et al. Prostate cancer localization using multiparametric MR imaging: comparison of Prostate Imaging Reporting and Data System (PI-RADS) and Likert scales. Radiology 2013; 269(2): 482–492. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
