

Cryoablation in lung transplantation: Its impact on pain, opioid use, and outcomes
- PMID: 37063121
- PMCID: PMC10091298
- DOI: 10.1016/j.xjon.2022.11.005
Cryoablation in lung transplantation: Its impact on pain, opioid use, and outcomes
Abstract
Objective: To assess the effect of intraoperative cryoablation on postoperative patient-reported pain, opioid use, and clinical outcomes in lung transplantation.
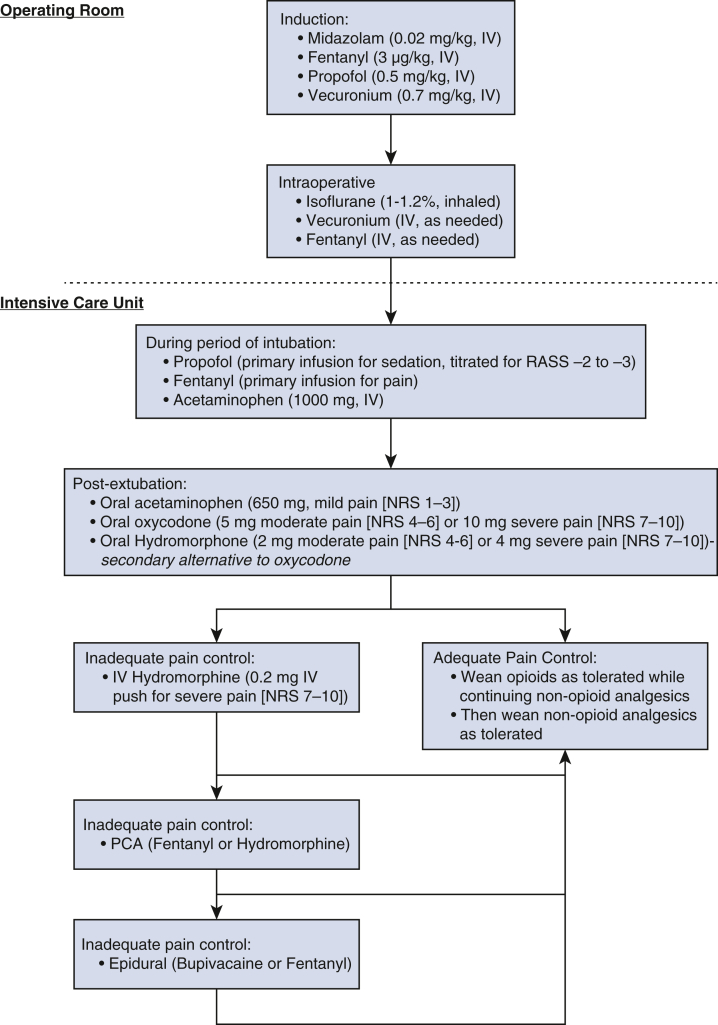
Methods: We performed a single-center retrospective cohort study of adult lung transplant recipients from August 2017 to September 2018. We compared outcomes of patients who received intraoperative cryoablation of the intercostal nerves with those who did not. Primary outcomes were postoperative patient-reported pain scores and opioid use. Secondary outcomes included postoperative sedation and agitation levels and perioperative outcomes. Data were abstracted from patients' electronic health records.
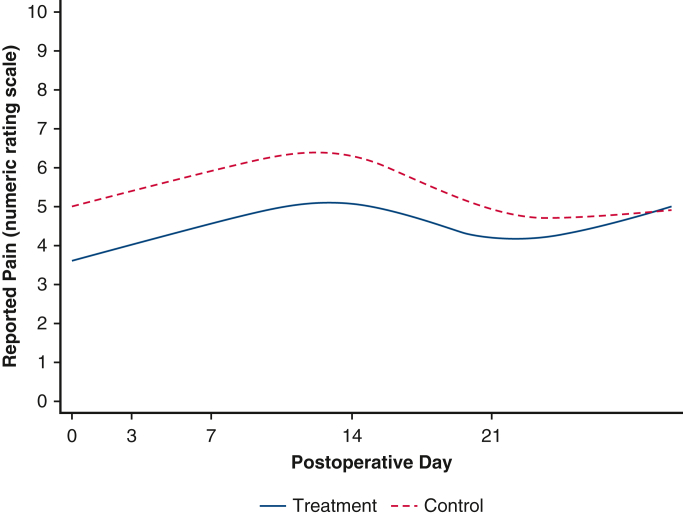
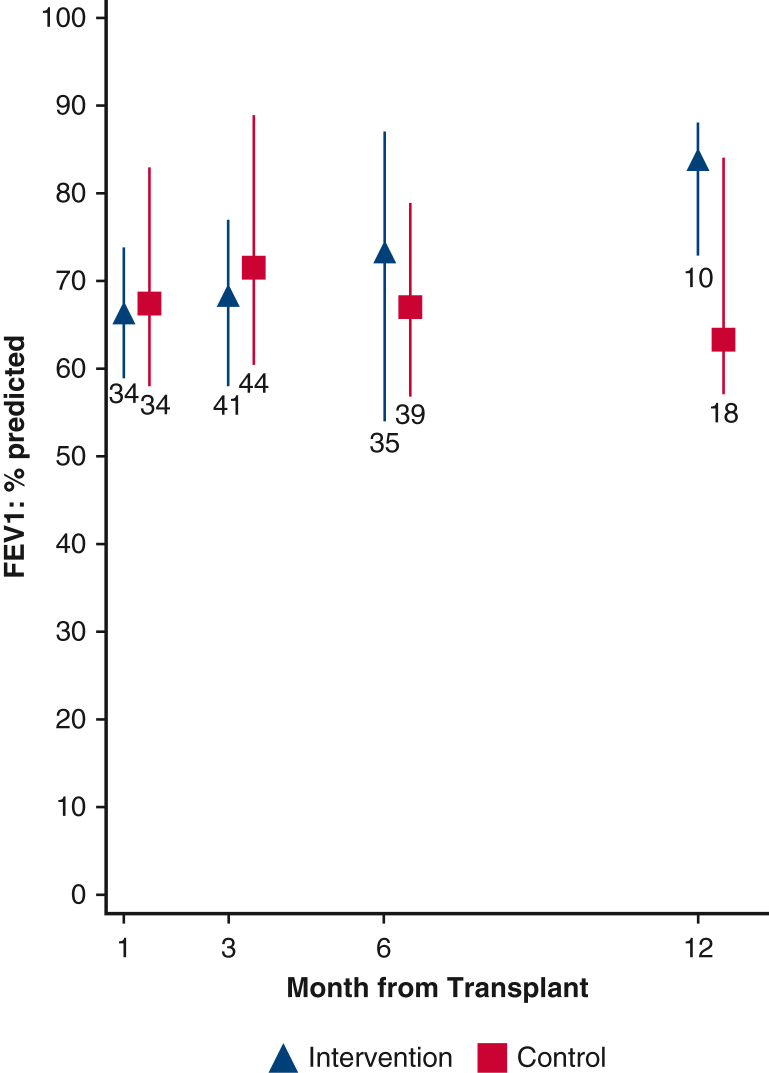
Results: Of the 102 patients transplanted, 45 received intraoperative cryoablation (intervention group) and 57 received the standard of care, which did not include intercostal or serratus blocks or immediate postoperative epidural placement (control group). The intervention group had significantly lower median and maximum postoperative pain scores at days 3 and 7 and significantly lower oral opioid use at days 3, 7, and 14 compared with the control group. Chronic opioid use at 3 and 6 months' posttransplant was lower in the intervention group. Differences in perioperative outcomes, including length of mechanical ventilation, sedation and agitation levels, and hospital stay, were not clinically meaningful. Survival at 30 days and 1 year was superior in the intervention compared with the control group.
Conclusions: Findings suggest that use of intraoperative cryoablation is an effective approach for treating pain and reducing opioid use in patients who undergo lung transplant, but a randomized study across multiple institutions is needed to confirm these findings.
Keywords: lung transplantation; pain; patient-reported outcomes.
Copyright © 2022 Published by Elsevier Inc.
Figures





References
-
- Farquhar J.M., Smith P.J., Snyder L., Gray A.L., Reynolds J.M., Blumenthal J.A. Patterns and predictors of pain following lung transplantation. Gen Hosp Psychiatr. 2018;50:125–130. - PubMed
-
- Richard C., Girard F., Ferraro P., Chouinard P., Boudreault D., Ruel M., et al. Acute postoperative pain in lung transplant recipients. Ann Thorac Surg. 2004;77:1951–1955. discussion 1955. - PubMed
-
- Schug S.A., Bruce J. Risk stratification for the development of chronic postsurgical pain. Schmerz. 2018;32:471–476. [in German] - PubMed
-
- Girard F., Chouinard P., Boudreault D., Poirier C., Richard C., Ruel M., et al. Prevalence and impact of pain on the quality of life of lung transplant recipients: a prospective observational study. Chest. 2006;130:1535–1540. - PubMed
LinkOut - more resources
Full Text Sources
Medical
