

Development and validation of a new prognostic immune-inflammatory-nutritional score for predicting outcomes after curative resection for intrahepatic cholangiocarcinoma: A multicenter study
- PMID: 37063918
- PMCID: PMC10102611
- DOI: 10.3389/fimmu.2023.1165510
Development and validation of a new prognostic immune-inflammatory-nutritional score for predicting outcomes after curative resection for intrahepatic cholangiocarcinoma: A multicenter study
Abstract
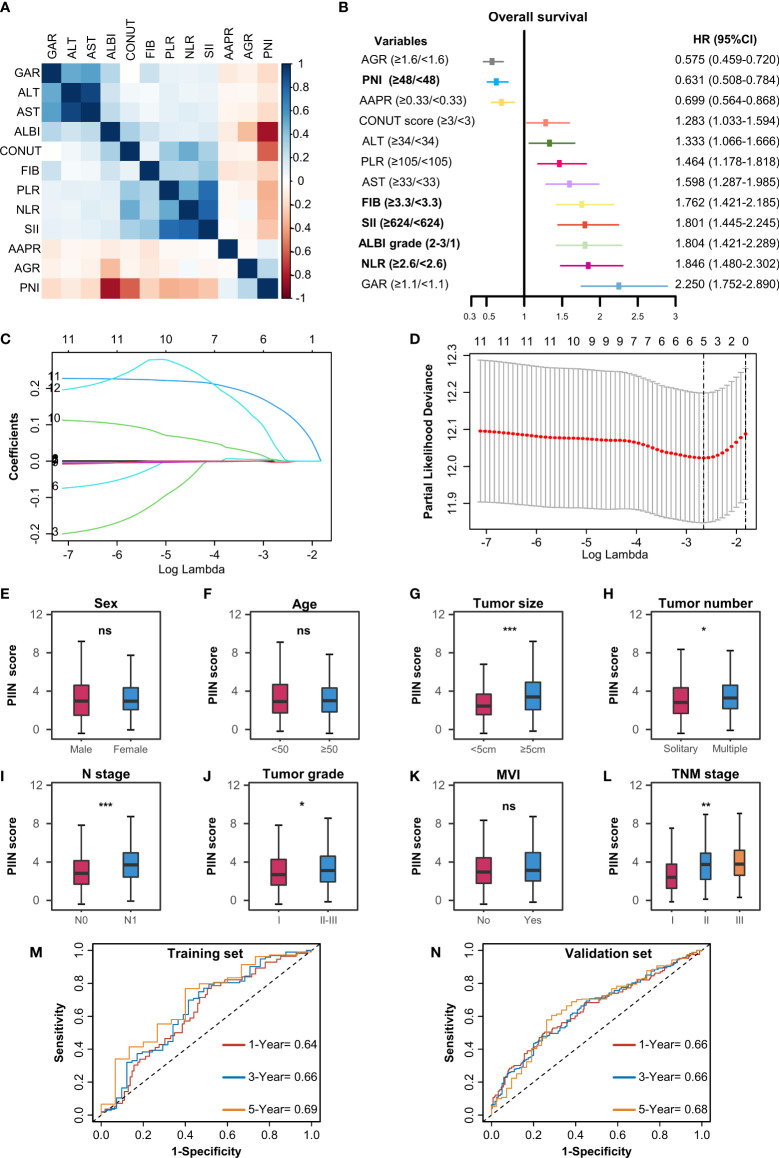
Background: Immune function, nutrition status, and inflammation influence tumor initiation and progression. This was a retrospective multicenter cohort study that investigated the prognostic value and clinical relevance of immune-, inflammatory-, and nutritional-related biomarkers to develop a novel prognostic immune-inflammatory-nutritional score (PIIN score) for patients with intrahepatic cholangiocarcinoma (ICC).
Methods: The clinical data of 571 patients (406 in the training set and 165 in the validation set) were collected from four large hepato-pancreatico-biliary centers of patients with ICC who underwent surgical resection between January 2011 and September 2017. Twelve blood biomarkers were collected to develop the PIIN score using the LASSO Cox regression model. The predictive value was further assessed using validation datasets. Afterward, nomograms combining the PIIN score and other clinicopathological parameters were developed and validated based on the calibration curve, time-dependent AUC curves, and decision curve analysis (DCA). The primary outcomes evaluated were overall survival (OS) and recurrence-free survival (RFS) from the day of primary resection of ICC.
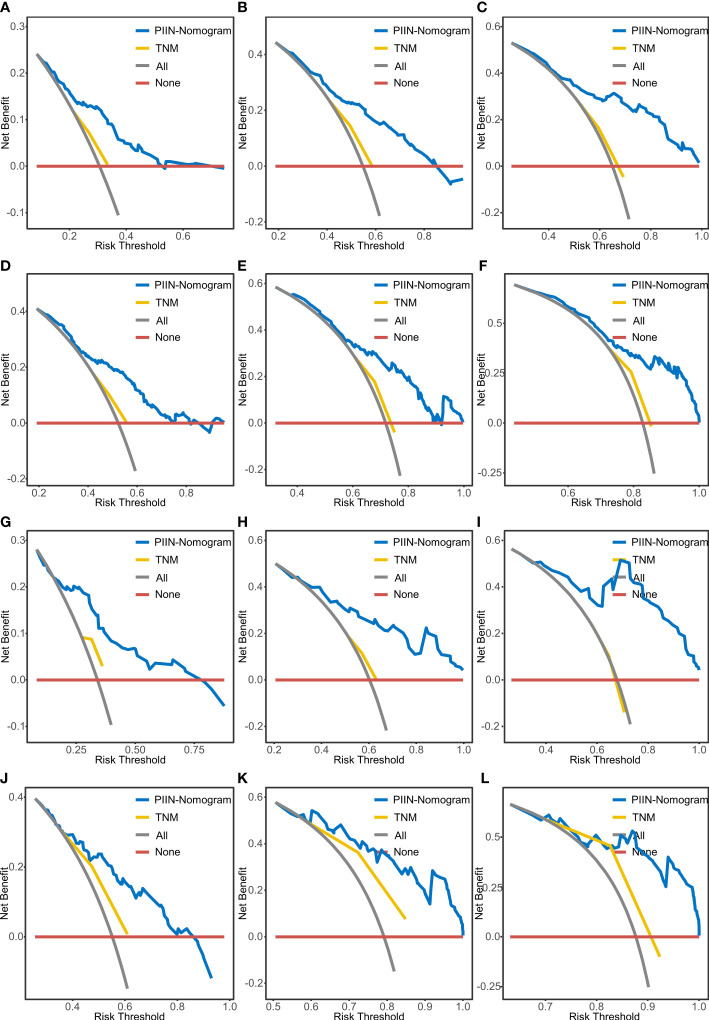
Results: Based on the albumin-bilirubin (ALBI) grade, neutrophil- to- lymphocyte ratio (NLR), prognostic nutritional index (PNI), and systemic immune- inflammation index (SII) biomarkers, the PIIN score that classified patients into high-risk and low-risk groups could be calculated. Patients with high-risk scores had shorter OS (training set, p < 0.001; validation set, p = 0.003) and RFS (training set, p < 0.001; validation set, p = 0.002) than patients with low-risk scores. The high PIIN score was also associated with larger tumors (≥5 cm), lymph node metastasis (N1 stage), multiple tumors, and high tumor grade or TNM (tumor (T), nodes (N), and metastases (M)) stage. Furthermore, the high PIIN score was a significant independent prognostic factor of OS and RFS in both the training (p < 0.001) and validation (p = 0.003) cohorts, respectively. A PIIN-nomogram for individualized prognostic prediction was constructed by integrating the PIIN score with the clinicopathological variables that yielded better predictive performance than the TNM stage.
Conclusion: The PIIN score, a novel immune-inflammatory-nutritional-related prognostic biomarker, predicts the prognosis in patients with resected ICC and can be a reliable tool for ICC prognosis prediction after surgery. Our study findings provide novel insights into the role of cancer-related immune disorders, inflammation, and malnutrition.
Keywords: immunity; inflammation; intrahepatic cholangiocarcinoma; nomogram; nutrition; prognosis.
Copyright © 2023 Zhu, Wang, Liu, Huang, Gao, Feng, Lan, Li and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical