

Case report: Primary pleural giant extraskeletal Ewing sarcoma in a child
- PMID: 37064103
- PMCID: PMC10102462
- DOI: 10.3389/fonc.2023.1137586
Case report: Primary pleural giant extraskeletal Ewing sarcoma in a child
Abstract
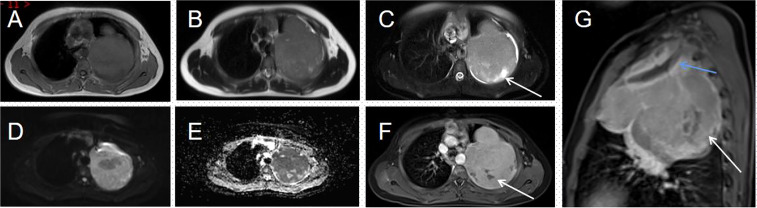
Primary extraskeletal Ewing sarcoma (EES) is a rare small round cell malignancy that accounts for less than 1% of all sarcomas. It is found most commonly in the trunk and lower limbs and very rarely in the pleura and can be easily misdiagnosed in clinical practice. This study presents the case of an 11-year-old boy who presented to our hospital with no apparent cause of left shoulder pain for 6 months. On physical examination, tenderness was noted in the left chest wall and shoulder joint, which had a limited range of motion. Computed tomography (CT) and magnetic resonance imaging (MRI) of the chest revealed an irregular soft tissue mass in the upper left thorax, with a wide base attached to the adjacent pleura and bone destruction of the adjacent left first rib. The patient's bone scan showed a dense focus of increased radiotracer accumulation in the left first rib. A subsequent CT-guided aspiration biopsy of the left pleural mass with histomorphology and immunohistochemical phenotyping led to a diagnosis of extraskeletal Ewing sarcoma. To inhibit tumor growth, alternating systemic chemotherapy cycles of vincristine, doxorubicin, and cyclophosphamide (VDC) and isocyclophosphamide and etoposide (IE) were administered at 3-week intervals. After completing three VDC and two IE cycles, the child's condition was well and the pain in the left shoulder joint was relieved. However, a repeat MRI of the chest showed that the mass did not shrink.
Keywords: case report; computed tomography; extraskeletal Ewing sarcoma; intrathoracic tumor; malignancy.
Copyright © 2023 Wu, Xie, Huang and Zhao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Rare origin - Ewing's sarcoma of the pleura: a case report and literature review.J Radiol Case Rep. 2023 Oct 31;17(10):21-25. doi: 10.3941/jrcr.v17i8.5187. eCollection 2023 Oct. J Radiol Case Rep. 2023. PMID: 38343883 Free PMC article. Review.
-
Extraskeletal Ewing Sarcoma of the Chest Wall Manifesting as a Palpable Breast Mass: Ultrasonography, CT, and MRI Findings.Taehan Yongsang Uihakhoe Chi. 2021 Jan;82(1):212-218. doi: 10.3348/jksr.2020.0109. Epub 2021 Jan 31. Taehan Yongsang Uihakhoe Chi. 2021. PMID: 36237473 Free PMC article.
-
A case of extraskeletal Ewing sarcoma originating from the visceral pleura.Hippokratia. 2011 Oct;15(4):363-5. Hippokratia. 2011. PMID: 24391423 Free PMC article.
-
Esophageal extraskeletal neoplasm Ewing's sarcoma: Case report.Int J Surg Case Rep. 2022 Aug;97:107399. doi: 10.1016/j.ijscr.2022.107399. Epub 2022 Jul 9. Int J Surg Case Rep. 2022. PMID: 35926382 Free PMC article.
-
Primary Ewing sarcoma of the larynx with distant metastasis: a case report and review of the literature.Curr Oncol. 2019 Aug;26(4):e574-e577. doi: 10.3747/co.26.5001. Epub 2019 Aug 1. Curr Oncol. 2019. PMID: 31548827 Free PMC article. Review.
Cited by
-
Rare Presentation of Primary Pleural Ewing Sarcoma With a Mass Extending Into the Right Ventricle: A Case Report.Cureus. 2024 Apr 3;16(4):e57542. doi: 10.7759/cureus.57542. eCollection 2024 Apr. Cureus. 2024. PMID: 38707066 Free PMC article.
-
Rare origin - Ewing's sarcoma of the pleura: a case report and literature review.J Radiol Case Rep. 2023 Oct 31;17(10):21-25. doi: 10.3941/jrcr.v17i8.5187. eCollection 2023 Oct. J Radiol Case Rep. 2023. PMID: 38343883 Free PMC article. Review.
-
Development and verification of prognostic nomogram for extraskeletal Ewing's sarcoma based on the SEER database.Heliyon. 2024 Nov 30;11(1):e40854. doi: 10.1016/j.heliyon.2024.e40854. eCollection 2025 Jan 15. Heliyon. 2024. PMID: 39801991 Free PMC article.
References
-
- Javery O, Krajewski K, Regan K, Kis B, Giardino A, Jagannathan J, et al. . A to z of extraskeletal Ewing sarcoma family of tumors in adults: Imaging features of primary disease, metastatic patterns, and treatment responses. AJR. Am J Roentgenol (2011) 197:W1015–1022. doi: 10.2214/AJR.11.6667 - DOI - PubMed
-
- Somarouthu BS, Shinagare AB, Rosenthal MH, Tirumani H, Hornick JL, Ramaiya NH, et al. . Multimodality imaging features, metastatic pattern and clinical outcome in adult extraskeletal Ewing sarcoma: Experience in 26 patients. Br J Radiol (2014) 87:20140123. doi: 10.1259/bjr.20140123 - DOI - PMC - PubMed
-
- Huh J, Kim KW, Park SJ, Kim HJ, Lee JS, Ha HK, et al. . Imaging features of primary tumors and metastatic patterns of the extraskeletal Ewing sarcoma family of tumors in adults: A 17-year experience at a single institution. Korean J Radiol (2015) 16:783–90. doi: 10.3348/kjr.2015.16.4.783 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources