

Systematic use of point of care ultrasound in neurosurgical intensive care unit: a practical approach
- PMID: 37064401
- PMCID: PMC10102800
- DOI: 10.21037/qims-22-667
Systematic use of point of care ultrasound in neurosurgical intensive care unit: a practical approach
Abstract
Background: Point of care ultrasound (POCUS) is a cost-effective, non-invasive procedure with high diagnostic reliability and therapeutic utilities. For various reasons, it is not being used routinely in neurosurgical intensive care unit (ICU). We have introduced a systematic use of POCUS in critically ill patients in our neurosurgical ICU. We have studied the various indications and benefit of using this technique.
Methods: This is a prospective, single center cohort observational study done in patients who were admitted in a tertiary neurosurgical ICU over 1 year (17th September 2020 to 16th September 2021). POCUS was used daily as per a standardized format for multiple purposes. A formal training to the operator was provided and standardized method of evaluation and intervention was used. Outcome was studied to understand the impact of the POCUS and difficulties encountered during its use.
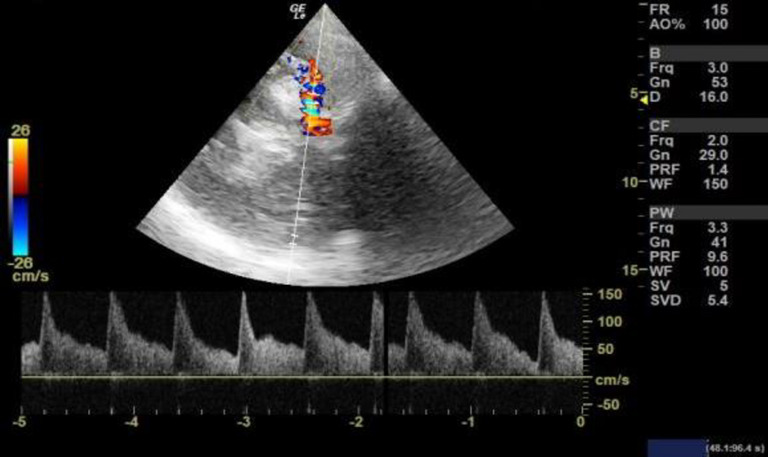
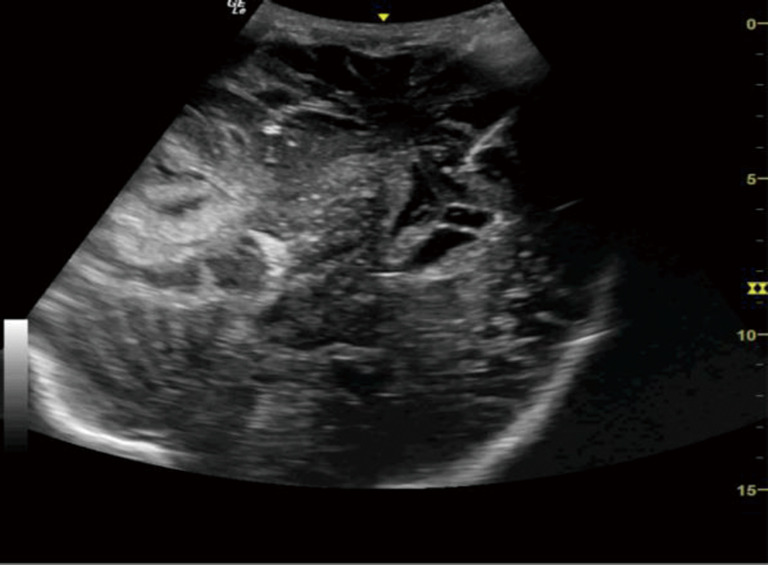
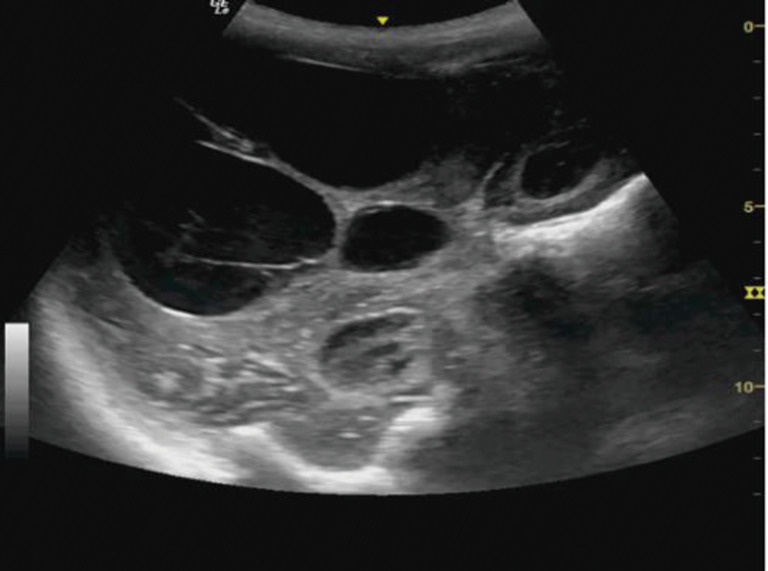
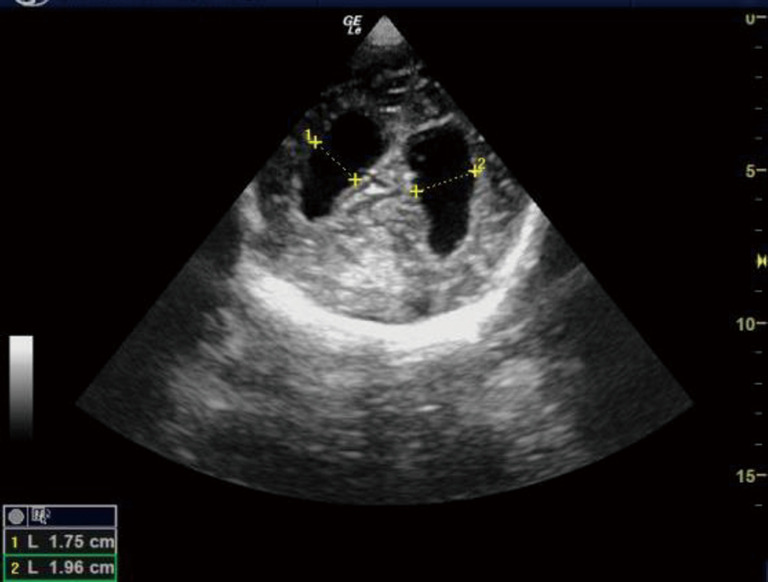
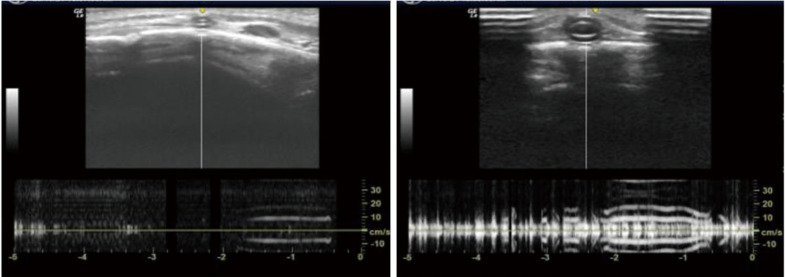
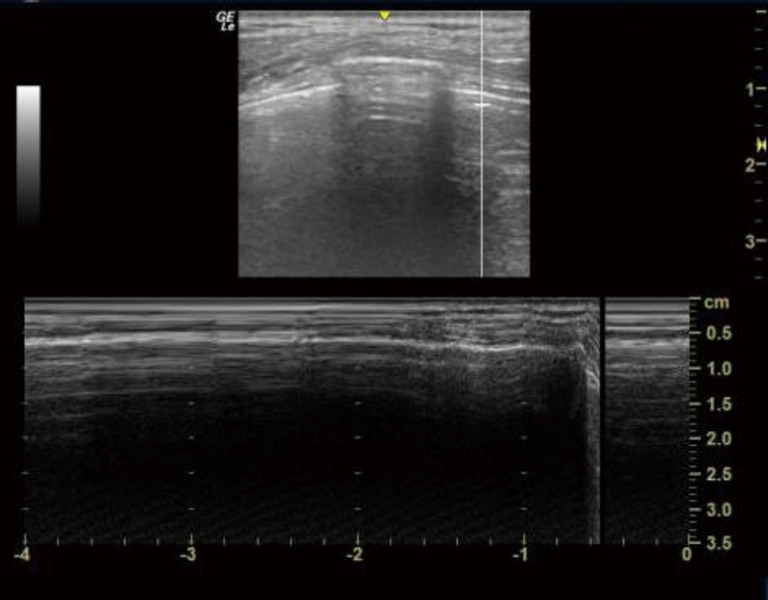
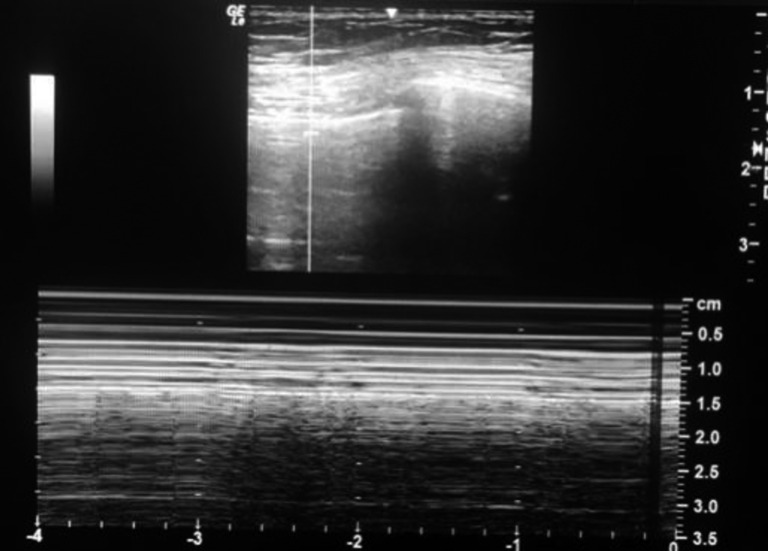
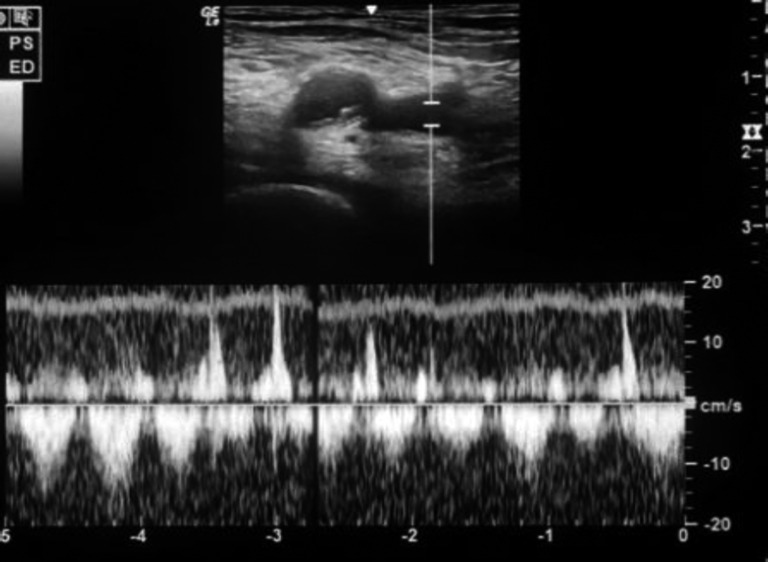
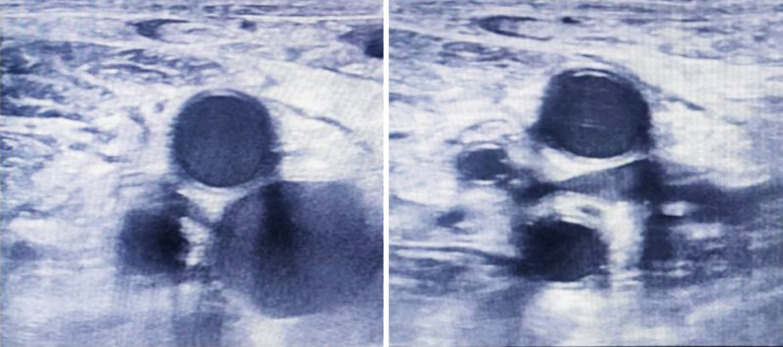
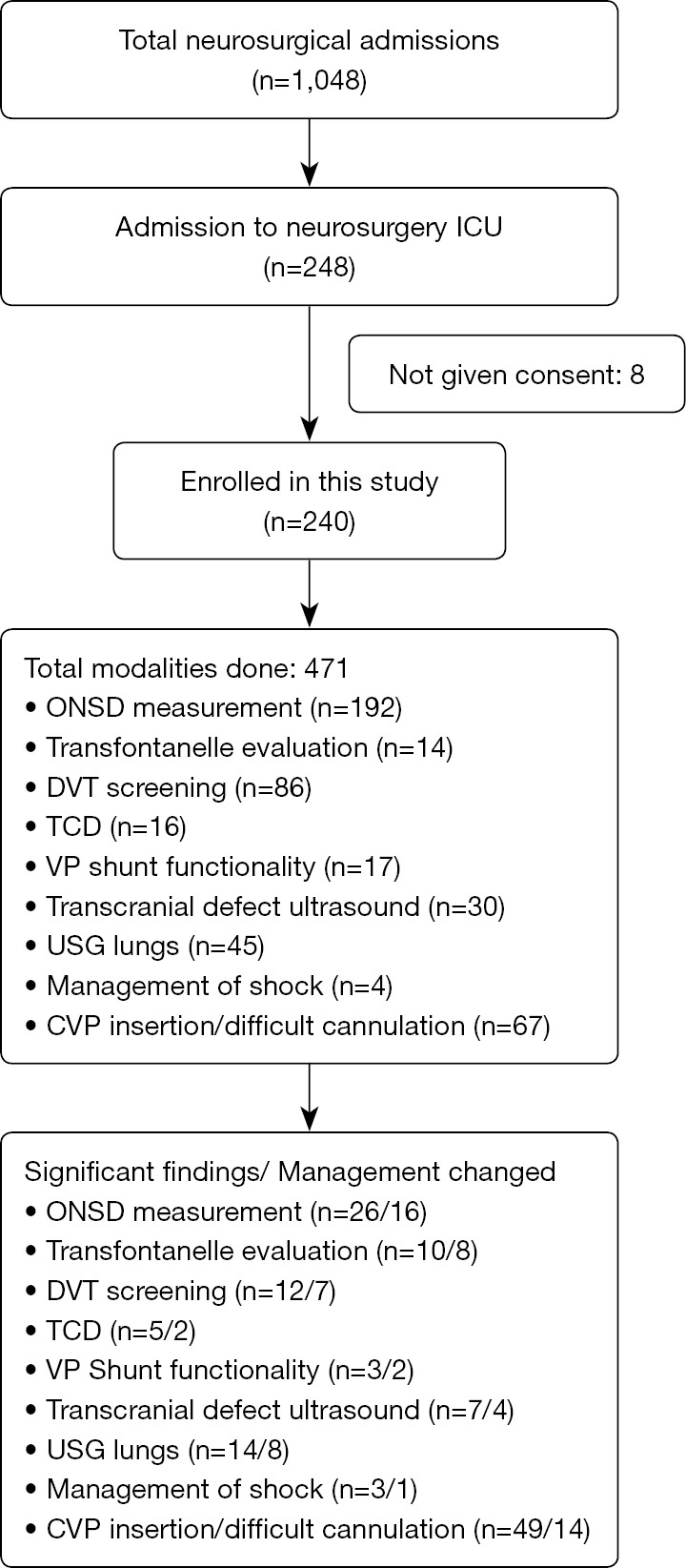
Results: POCUS was used in 240 patients, including all patients for primary and secondary surveys, 192 patients (80%) for optic nerve sheath diameter (ONSD) measurement, 14 myelomeningoceles for trans-fontanelle ultrasound study, 16 post operative cases of aneurysm clipping for transcranial Doppler (TCD) study, 86 patients for deep vein thrombosis (DVT) screening, 17 for evaluation of ventriculo-peritoneal (VP) shunt functionality, 30 for transcranial defect ultrasound, 45 for chest ultrasound, 4 for evaluation of hemodynamic shock and 67 patients who had difficult cannualtion or while insertion of central venous catheter placement. POCUS was also used for difficult cannulation, central catheter placement and e-FAST scan. Significant findings were reported 129 times, which led to immediate change in management in 62 patients (25.83%) as compared to 16 patients in whom significant findings were not reported using POCUS, but management was changed using other radiological modalities (P<0.01). There was initial lag in adopting the technique, however with practice, the team developed confidence. As a result, the accuracy and time taken to perform the procedure was reduced significantly.
Conclusions: Routine systematic use of POCUS can be beneficial not only for the rapid diagnosis and prompt management of patients, but also helpful in monitoring and performing various procedures in neurosurgical ICU. Though not all modalities mentioned in standardized format was used in all patients, use of this format has helped improved training and maintain proper use of POCUS in our ICU.
Keywords: Point of care ultrasound (POCUS); neurosurgical intensive care unit (ICU); sonoscopy; ultrasonography (USG).
2023 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-22-667/coif). The authors have no conflicts of interest to declare.
Figures




Comment in
-
Systematic use of standardized A-scan technique in neurosurgical intensive care unit.Quant Imaging Med Surg. 2023 Oct 1;13(10):7396-7397. doi: 10.21037/qims-23-628. Epub 2023 Jul 7. Quant Imaging Med Surg. 2023. PMID: 37869285 Free PMC article. No abstract available.
References
-
- Robba C, Goffi A, Geeraerts T, Cardim D, Via G, Czosnyka M, Park S, Sarwal A, Padayachy L, Rasulo F, Citerio G. Brain ultrasonography: methodology, basic and advanced principles and clinical applications. A narrative review. Intensive Care Med 2019;45:913-27. 10.1007/s00134-019-05610-4 - DOI - PubMed
-
- Loomis AL, Chakko MN. Doppler Trans-Cranial Assessment, Protocols, And Interpretation. In: StatPearls. Treasure Island, FL, USA: StatPearls Publishing, 2022. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials