

Dehiscence of colorectal anastomosis treated with noninvasive procedures
- PMID: 37064554
- PMCID: PMC10091912
- DOI: 10.5114/wiitm.2022.121701
Dehiscence of colorectal anastomosis treated with noninvasive procedures
Abstract
Introduction: Most postoperative rectal leakages can be successfully treated with minimally invasive procedures. Endoscopic vacuum therapy supported by tissue adhesives or cellular growth stimulants closes even chronic anastomotic fistulas.
Aim: To present a treatment strategy for postoperative leakage of rectal anastomoses with noninvasive procedures.
Material and methods: From 2015 to 2020, a group of 25 patients with postoperative rectal leakage was enrolled for minimally invasive treatment. The indication for the therapy was anastomotic dehiscence not exceeding 1/2 of the bowel circuit and the absence of severe septic complications. All patients were healed with endoluminal vacuum therapy (EVT) supported by hemostatic clips, tissue adhesives or cellular growth stimulants.
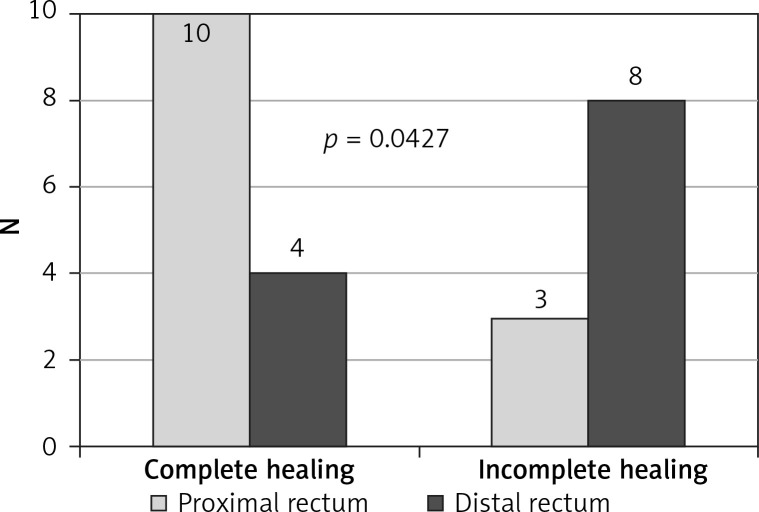
Results: Complete drainage and reduction of leakage were achieved in 23 patients. The fistula was totally closed in 21 patients and in 2 of them it was restricted to a slit sinus. Two patients required revision surgery. Endoscopic treatment attempted within 7 days from leakage detection, as well as the size of the dehiscence less than 1/4 of the bowel circuit, increased the chance of full healing. In contrast, ultra low resection and neoadjuvant radiotherapy impaired the healing process, limiting the effectiveness of noninvasive therapy.
Conclusions: The minimally invasive approach successfully restricts anastomotic leakage and reduces the diameter of dehiscence. Early initiation of the therapy and the size of rupture determine the final results. The use of complementary endoscopic solutions, such as clips or tissue adhesives, increases the effectiveness of the noninvasive strategy.
Keywords: anastomotic dehiscence; endoluminal vacuum therapy; noninvasive treatment; rectal leak; tissue adhesive.
Copyright: © 2022 Fundacja Videochirurgii.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
Minimally invasive treatment of postoperative fistulas, leakages, and perforations of the upper gastrointestinal tract: a single-center observational study.Wideochir Inne Tech Maloinwazyjne. 2023 Dec;18(4):655-664. doi: 10.5114/wiitm.2023.133838. Epub 2023 Dec 18. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 38239587 Free PMC article.
-
Transrectal endoscopic drainage with vacuum-assisted therapy in patients with anastomotic leaks following rectal cancer resection.Surg Endosc. 2022 Feb;36(2):959-967. doi: 10.1007/s00464-021-08359-4. Epub 2021 Mar 1. Surg Endosc. 2022. PMID: 33650007 Free PMC article.
-
Influence of Neoadjuvant Therapy on Success of Endoscopic Vacuum Therapy in Anastomotic Leakage after Rectal Resection Because of Rectal Cancer.J Clin Med. 2024 Jul 8;13(13):3982. doi: 10.3390/jcm13133982. J Clin Med. 2024. PMID: 38999546 Free PMC article.
-
Systematic review of endoluminal vacuum-assisted therapy as salvage treatment for rectal anastomotic leakage.BJS Open. 2018 Dec 26;3(2):153-160. doi: 10.1002/bjs5.50124. eCollection 2019 Apr. BJS Open. 2018. PMID: 30957061 Free PMC article.
-
Postoperative non-steroidal anti-inflammatory drugs and colorectal anastomotic leakage. NSAIDs and anastomotic leakage.Dan Med J. 2012 Mar;59(3):B4420. Dan Med J. 2012. PMID: 22381097 Review.
Cited by
-
Minimally invasive treatment of postoperative fistulas, leakages, and perforations of the upper gastrointestinal tract: a single-center observational study.Wideochir Inne Tech Maloinwazyjne. 2023 Dec;18(4):655-664. doi: 10.5114/wiitm.2023.133838. Epub 2023 Dec 18. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 38239587 Free PMC article.
References
-
- Daams F, Slieker JC, Tedja A, et al. . Treatment of colorectal anastomotic leakage: results of a questionnaire amongst members of the Dutch Society of Gastrointestinal Surgery. Dig Surg 2012; 29: 516-21. - PubMed
-
- Rullier E, Laurent C, Garrelon JL, et al. . Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 1998; 85: 355-8. - PubMed
LinkOut - more resources
Full Text Sources