

A Case of Septic Pulmonary Embolism Caused by Pyelonephritis With Klebsiella pneumoniae in a Patient With Poorly Controlled Type 2 Diabetes Mellitus
- PMID: 37065415
- PMCID: PMC10097463
- DOI: 10.7759/cureus.36098
A Case of Septic Pulmonary Embolism Caused by Pyelonephritis With Klebsiella pneumoniae in a Patient With Poorly Controlled Type 2 Diabetes Mellitus
Abstract
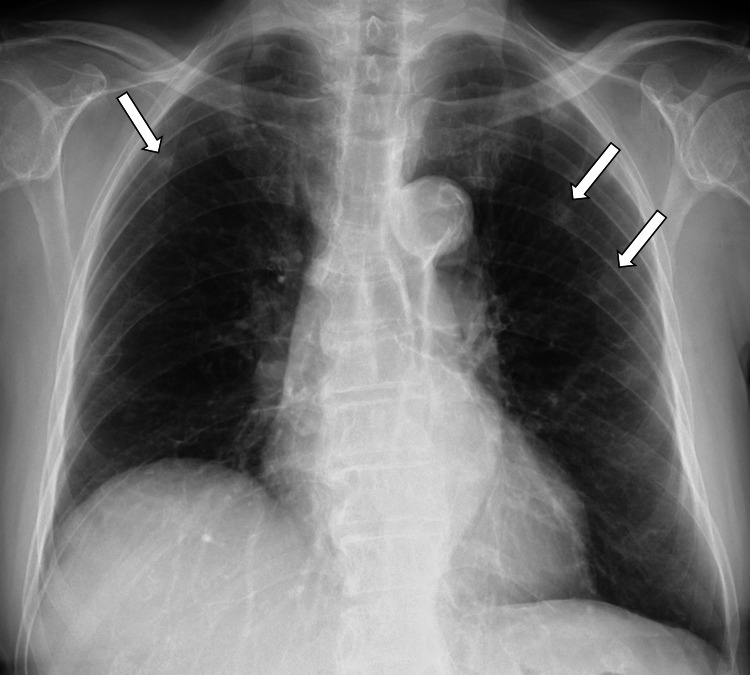
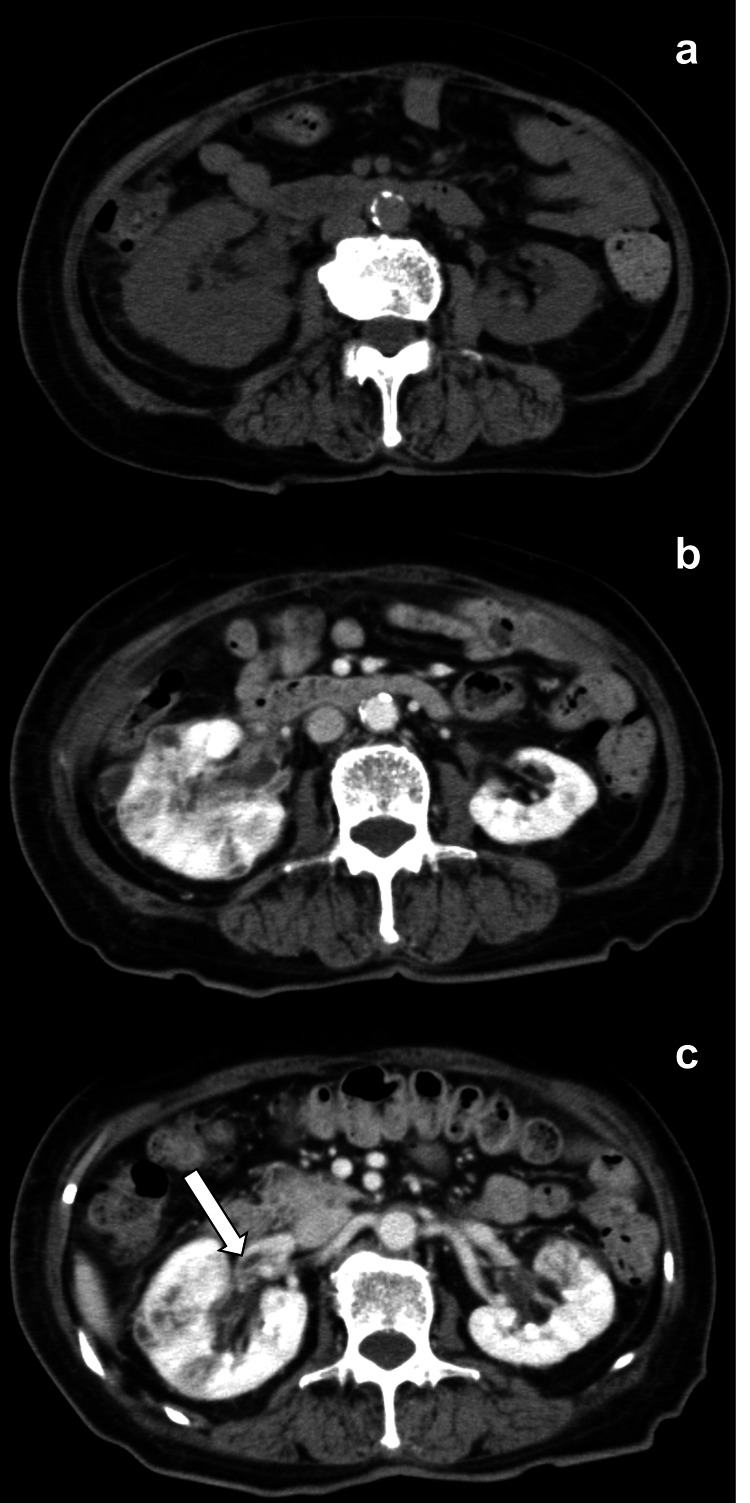
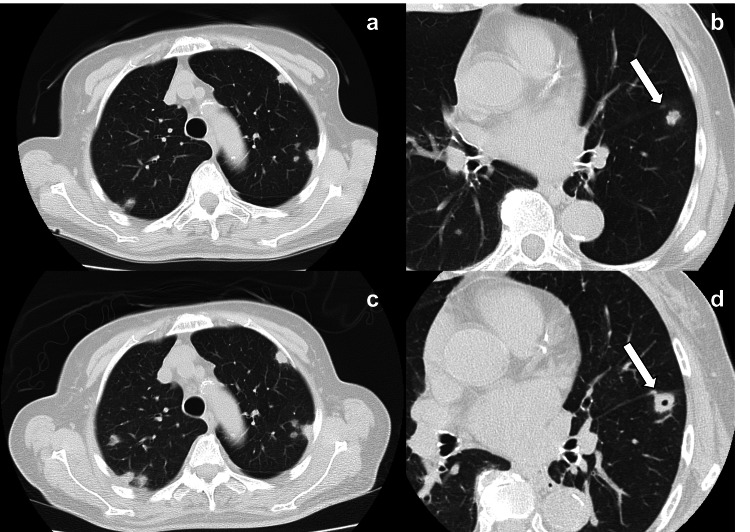
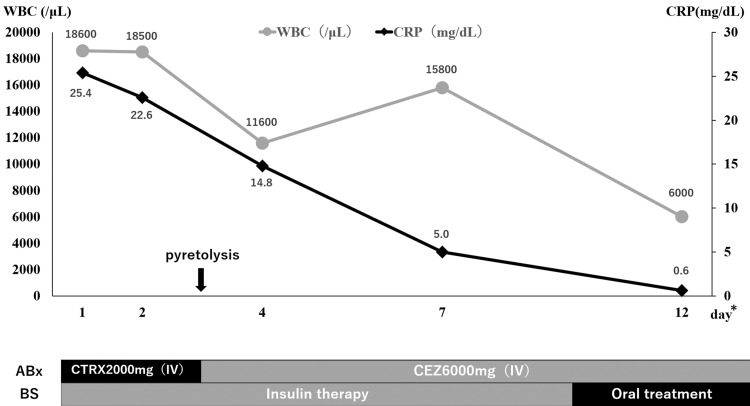
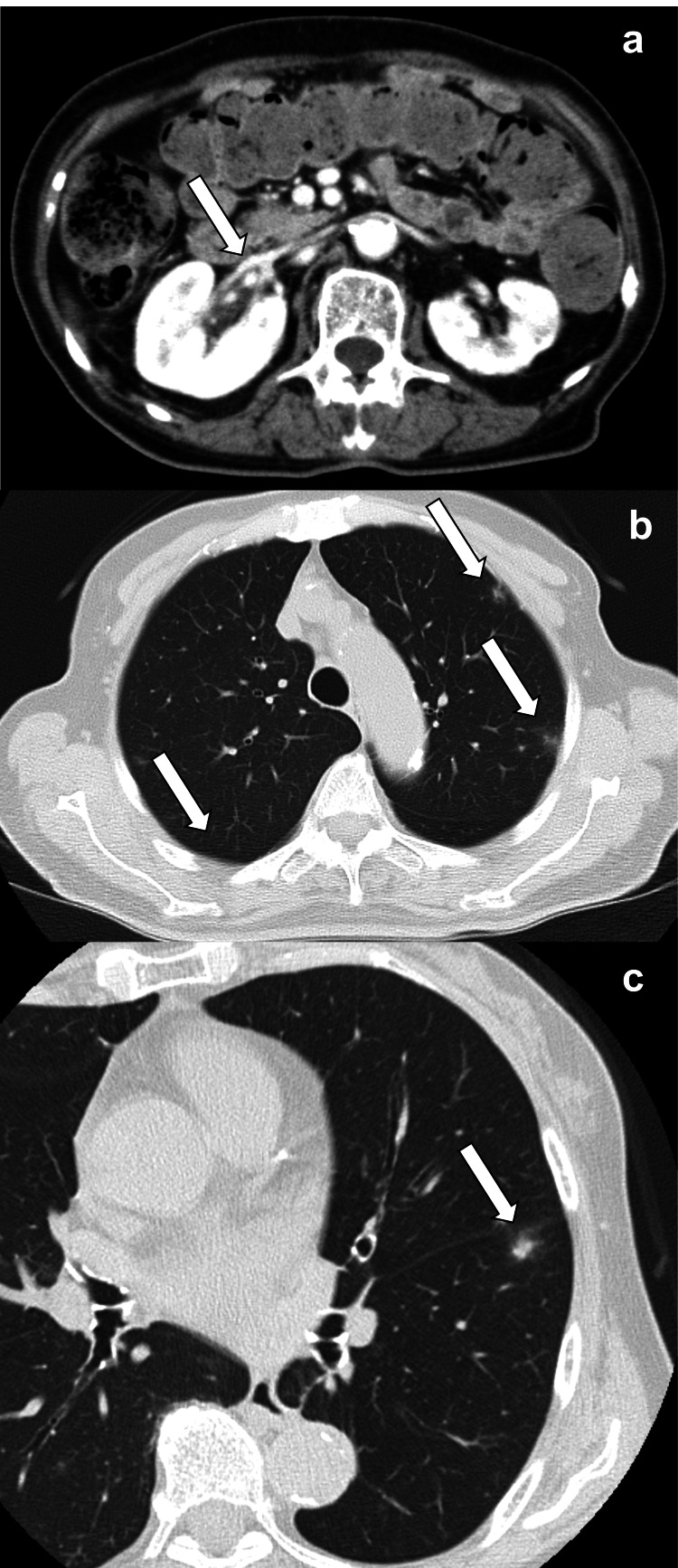
Septic pulmonary embolism (SPE) is caused by the microbe that is responsible for any clinical condition that may include urinary tract infections as in this case. We report a case of pyelonephritis with Klebsiella pneumoniae that led to SPE in an 80-year-old woman with poorly controlled diabetes mellitus (DM). Computed tomography (CT) revealed multiple nodules in the peripheral area of the bilateral lung and a contrast defect in the right renal vein, which was suspected to be an embolism. Blood and urine cultures revealed Klebsiella pneumoniae infection. These results confirmed the diagnosis of pyelonephritis and SPE. Treatment with ceftriaxone, cefazolin, and ciprofloxacin improved the patient's condition.
Keywords: klebsiella pneumoniae (kp); poorly controlled diabetes; septic pulmonary emboli; type 2 diabetes mellitus (dm); urinary tract infection.
Copyright © 2023, Katsumata et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Septic pulmonary embolism: presenting features and clinical course of 14 patients. Cook RJ, Ashton RW, Aughenbaugh GL, Ryu JH. Chest. 2005;128:162–166. - PubMed
-
- Klebsiella pneumoniae infection associated septic pulmonary embolism in an emergency department from east China. Zhang X, Yang Q, Gao B, et al. Ann Palliat Med. 2021;10:1521–1529. - PubMed
-
- Pulmonary septic emboli: diagnosis with CT. Kuhlman JE, Fishman EK, Teigen C. Radiology. 1990;174:211–213. - PubMed
Publication types
LinkOut - more resources
Full Text Sources