

One hundred cases of primary spontaneous pneumomediastinum: leukocytosis is common, pleural effusions and age over 40 are rare
- PMID: 37065555
- PMCID: PMC10089890
- DOI: 10.21037/jtd-22-1136
One hundred cases of primary spontaneous pneumomediastinum: leukocytosis is common, pleural effusions and age over 40 are rare
Abstract
Background: Primary spontaneous pneumomediastinum (PSPM) is a benign condition, but it can be difficult to discriminate from Boerhaave syndrome. The diagnostic difficulty is attributable to a shared constellation of history, signs, and symptoms combined with a poor understanding of the basic vital signs, labs, and diagnostic findings characterizing PSPM. These challenges likely contribute to high resource utilization for diagnosis and management of a benign process.
Methods: Patients aged 18 years or older with PSPM were identified from our radiology department's database. A retrospective chart review was performed.
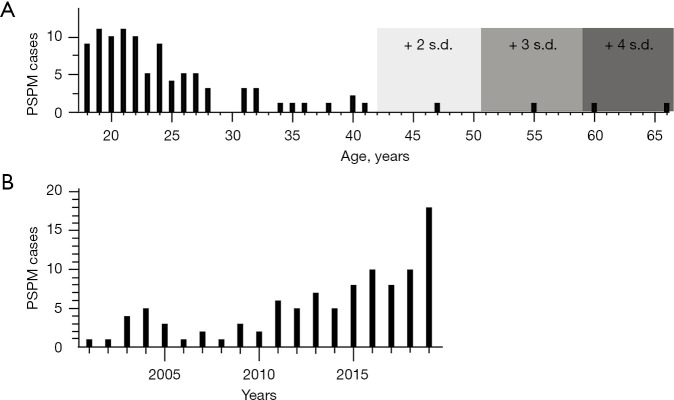
Results: Exactly 100 patients with PSPM were identified between March 2001 and November 2019. Demographics and histories correlated well with prior studies: mean age (25 years); male predominance (70%); association with cough (34%), asthma (27%), retching or emesis (24%), tobacco abuse (11%), and physical activity (11%); acute chest pain (75%), and dyspnea (57%) as the first and second most frequent symptoms and subcutaneous emphysema (33%) as the most common sign. We provide the first robust data on presenting vital signs and laboratory values of PSPM, showing that tachycardia (31%) and leukocytosis (30%) were common. No pleural effusion was found in the 66 patients who underwent computed tomography (CT) of the chest. We provide the first data on inter-hospital transfer rates (27%). 79% of transfers were due to concern for esophageal perforation. Most patients were admitted (57%), with an average length of stay (LOS) of 2.3 days, and 25% received antibiotics.
Conclusions: PSPM patients frequently present in their twenties with chest pain, subcutaneous emphysema, tachycardia, and leukocytosis. Approximately 25% have a history of retching or emesis and it is this population that must be discriminated from those with Boerhaave syndrome. An esophagram is rarely indicated and observation alone is appropriate in patients under age 40 with a known precipitating event or risk factors for PSPM (e.g., asthma, smoking) if they have no history of retching or emesis. Fever, pleural effusion, and age over 40 are rare in PSPM and should raise concern for esophageal perforation in a patient with a history of retching, emesis, or both.
Keywords: Boerhaave syndrome; Pneumomediastinum; esophageal perforation.
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1136/coif). DPM has received financial remuneration for consulting services from Atricure and Cook Medical, and for advisory board participation from Lung Bioengineering and Atricure. DPM has grant funding from Ethicon. None of these conflicts have any relevance to the content of this manuscript. The other authors have no conflicts of interest to declare.
Figures

References
-
- Hamman L. Spontaneous mediastinal emphysema. Bull Johns Hopkins Hosp 1939;64:1-21.
-
- Macklin MT, Macklin CC. Malignant interstitial emphysema of the lungs and mediastinum as an important occult complication in many respiratory diseases and other conditions: an interpretation of the clinical literature in the light of laboratory experiment. Medicine (Baltimore) 1944;23:281-358. 10.1097/00005792-194412000-00001 - DOI
LinkOut - more resources
Full Text Sources