

Multi-level analysis and evaluation of organizational improvements in thoracic surgery according to a Value-Based HealthCare approach
- PMID: 37065599
- PMCID: PMC10089880
- DOI: 10.21037/jtd-22-1294
Multi-level analysis and evaluation of organizational improvements in thoracic surgery according to a Value-Based HealthCare approach
Abstract
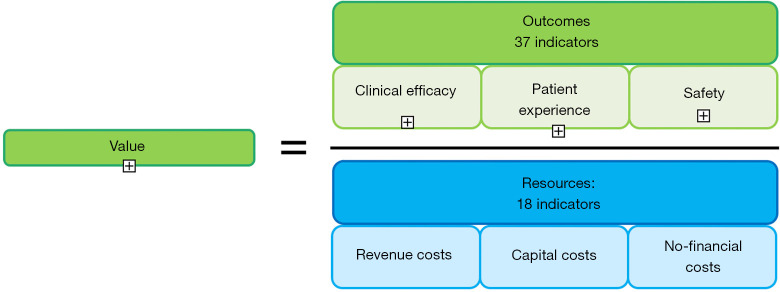
Background: Value-Based HealthCare (VBHC), designed by Harvard University, is an evolving model of healthcare delivery that achieves better patient outcomes and greater financial sustainability for the healthcare professionals. According to this innovative approach, the value is determined by a panel of indicators and the ratio between results and costs. Our goal was to develop a panel of thoracic-fashioned key-performance indicators (KPIs) creating a model that could be applied in thoracic surgery for the first time, reporting our early experience.
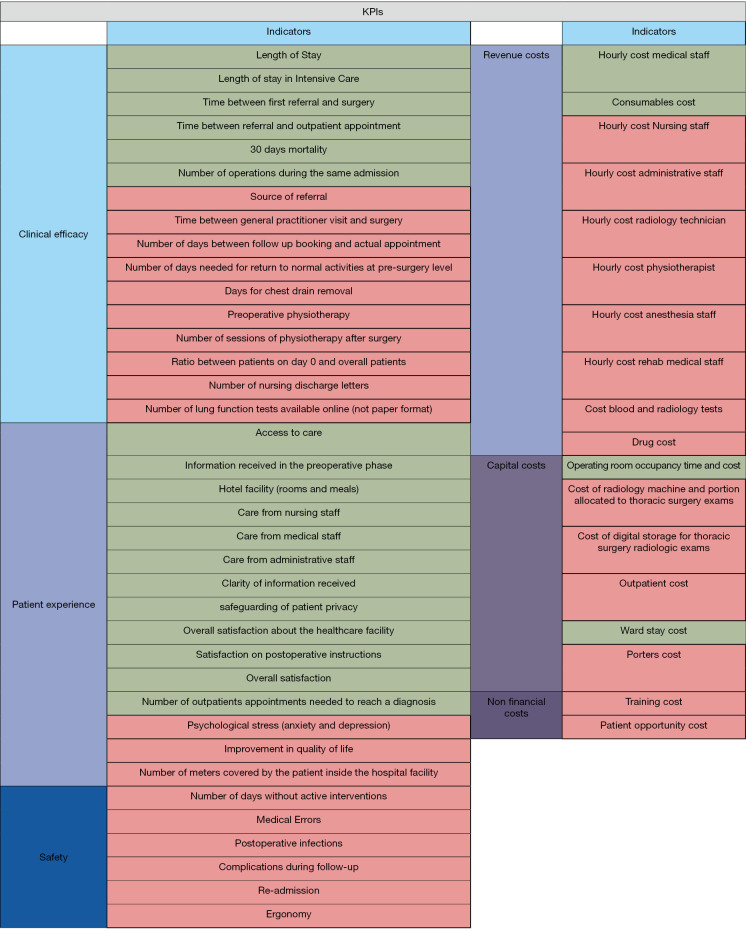
Methods: Fifty-five indicators were developed based on literature review: 37 for outcomes and 18 for costs. Outcomes were measured by a 7 level Likert scale, while overall costs were defined through the sum of the individual economic performance on each resource indicator. An observational retrospective cross-sectional study was designed to make a cost-effective evaluation of the indicators. Therefore, the Patient Value in Thoracic Surgery (PVTS) score calculated value gained for every lung cancer patient undergoing lung resection at our surgical department.
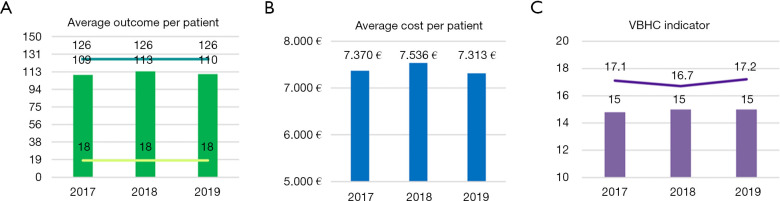
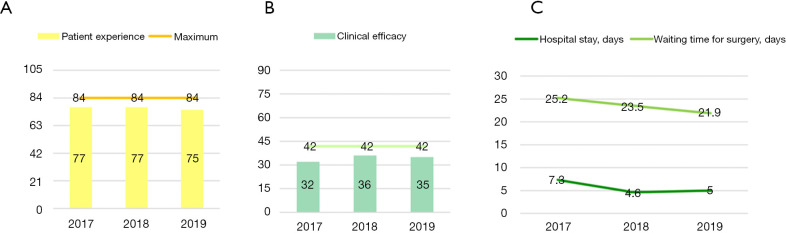
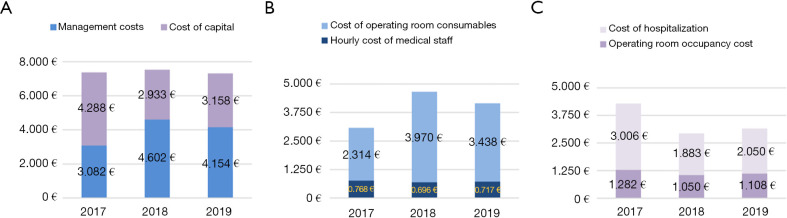
Results: A total of 552 patients were enrolled. From 2017 to 2019 mean outcome indicators per patient were 109, 113 and 110 while mean costs per patient were 7.370, 7.536 and 7.313 euros respectively. Hospital stay and waiting time from consultation to surgery for lung cancer patients decreased from 7.3 to 5 and from 25.2 to 21.9 days, respectively. On the contrary, number of patients increased but overall costs decreased, despite cost of consumables has gone from 2.314 to 3.438 euros, since cost of hospitalization and occupancy of the operating room (OR) improved (from 4.288 to 3.158 euros). Variables analyzed showed that overall value delivered grew from 14.8 to 15.
Conclusions: Introducing a new concept of value, the VBHC theory applied to thoracic surgery may revolutionize traditional organizational management in lung cancer patients, showing how value delivered can increase in accordance with outcomes, despite the growth of part of the costs. Our panel of indicators has been created to provide an innovative score to successfully identify improvements needed and quantify their effectiveness in Thoracic Surgery and our early experience reports encouraging results.
Keywords: Thoracic surgery; Value-Based HealthCare (VBHC); enhanced recovery after surgery (ERAS); key performance indicators (KPIs); patient-centered care.
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1294/coif). PF serves as an unpaid editorial board member of Journal of Thoracic Disease from October 2022 to September 2024. The other authors have no conflicts of interest to declare.
Figures
Comment in
-
Measuring costs and outcomes: what are suitable models while implementing value-based healthcare in thoracic surgery?J Thorac Dis. 2023 Dec 30;15(12):6395-6402. doi: 10.21037/jtd-23-1364. Epub 2023 Dec 19. J Thorac Dis. 2023. PMID: 38249893 Free PMC article. No abstract available.
Similar articles
-
Healthcare can't stop evolving: innovation as the catalyst for unleashing the managerial potential of value-based healthcare by stimulating intangible assets and enhancing organizational resilience.Front Psychol. 2024 Sep 19;15:1438029. doi: 10.3389/fpsyg.2024.1438029. eCollection 2024. Front Psychol. 2024. PMID: 39364090 Free PMC article. Review.
-
Enhancing the value of the oncology thoracic surgery care pathway: a TDABC and ABC analysis.BMC Health Serv Res. 2024 Oct 28;24(1):1294. doi: 10.1186/s12913-024-11829-9. BMC Health Serv Res. 2024. PMID: 39468543 Free PMC article.
-
Endovascular stent grafting and open surgical replacement for chronic thoracic aortic aneurysms: a systematic review and prospective cohort study.Health Technol Assess. 2022 Jan;26(6):1-166. doi: 10.3310/ABUT7744. Health Technol Assess. 2022. PMID: 35094747
-
Value-based preoperative assessment in a large academic hospital.J Anesth Analg Crit Care. 2024 Jul 8;4(1):42. doi: 10.1186/s44158-024-00161-7. J Anesth Analg Crit Care. 2024. PMID: 38978057 Free PMC article.
-
Toward a Clearer Understanding of Value-Based Healthcare: A Concept Analysis.J Nurs Manag. 2025 Apr 19;2025:8186530. doi: 10.1155/jonm/8186530. eCollection 2025. J Nurs Manag. 2025. PMID: 40343256 Free PMC article. Review.
Cited by
-
Implementing value-based healthcare: a scoping review of key elements, outcomes, and challenges for sustainable healthcare systems.Front Public Health. 2025 Apr 9;13:1514098. doi: 10.3389/fpubh.2025.1514098. eCollection 2025. Front Public Health. 2025. PMID: 40270723 Free PMC article.
-
Measuring costs and outcomes: what are suitable models while implementing value-based healthcare in thoracic surgery?J Thorac Dis. 2023 Dec 30;15(12):6395-6402. doi: 10.21037/jtd-23-1364. Epub 2023 Dec 19. J Thorac Dis. 2023. PMID: 38249893 Free PMC article. No abstract available.
References
-
- Porter ME, Teisberg EO. Redefining Health Care: Creating Value-Based Competition on Results. 2006 Boston, MA: Harvard Business School Press.
-
- Porter M, Lee TH. The strategy that will fix health care. Harv Bus Rev 2013;91:50-705. - PubMed
LinkOut - more resources
Full Text Sources