

Prediction models for respiratory outcomes in patients with COVID-19: integration of quantitative computed tomography parameters, demographics, and laboratory features
- PMID: 37065603
- PMCID: PMC10089866
- DOI: 10.21037/jtd-22-1076
Prediction models for respiratory outcomes in patients with COVID-19: integration of quantitative computed tomography parameters, demographics, and laboratory features
Abstract
Background: We aimed to develop integrative machine-learning models using quantitative computed tomography (CT) parameters in addition to initial clinical features to predict the respiratory outcomes of coronavirus disease 2019 (COVID-19).
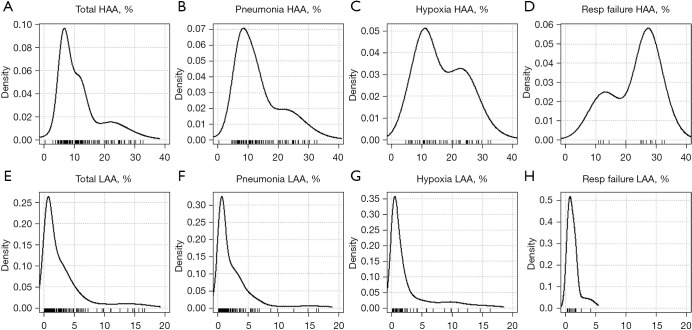
Methods: This was a retrospective study involving 387 patients with COVID-19. Demographic, initial laboratory, and quantitative CT findings were used to develop predictive models of respiratory outcomes. High-attenuation area (HAA) (%) and consolidation (%) were defined as quantified percentages of the area with Hounsfield units between -600 and -250 and between -100 and 0, respectively. Respiratory outcomes were defined as the development of pneumonia, hypoxia, or respiratory failure. Multivariable logistic regression and random forest models were developed for each respiratory outcome. The performance of the logistic regression model was evaluated using the area under the receiver operating characteristic curve (AUC). The accuracy of the developed models was validated by 10-fold cross-validation.
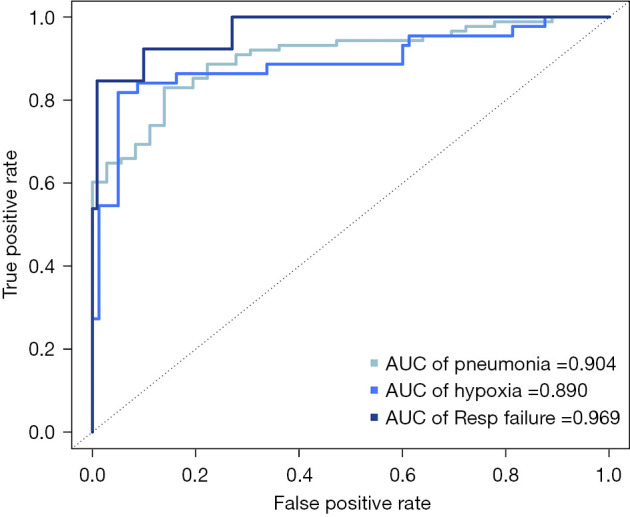
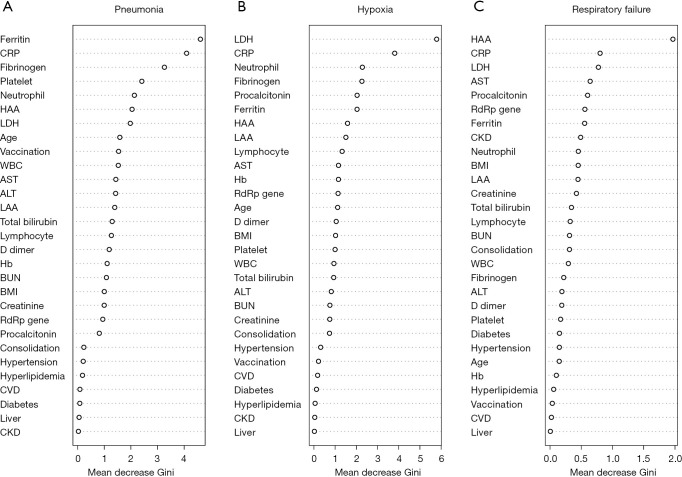
Results: A total of 195 (50.4%), 85 (22.0%), and 19 (4.9%) patients developed pneumonia, hypoxia, and respiratory failure, respectively. The mean patient age was 57.8 years, and 194 (50.1%) were female. In the multivariable analysis, vaccination status and levels of lactate dehydrogenase, C-reactive protein (CRP), and fibrinogen were independent predictors of pneumonia. The presence of hypertension, levels of lactate dehydrogenase and CRP, HAA (%), and consolidation (%) were selected as independent variables to predict hypoxia. For respiratory failure, the presence of diabetes, levels of aspartate aminotransferase, and CRP, and HAA (%) were selected. The AUCs of the prediction models for pneumonia, hypoxia, and respiratory failure were 0.904, 0.890, and 0.969, respectively. Using the feature selection in the random forest model, HAA (%) was ranked as one of the top 10 features predicting pneumonia and hypoxia and was first place for respiratory failure. The accuracies of the cross-validation of the random forest models using the top 10 features for pneumonia, hypoxia, and respiratory failure were 0.872, 0.878, and 0.945, respectively.
Conclusions: Our prediction models that incorporated quantitative CT parameters into clinical and laboratory variables showed good performance with high accuracy.
Keywords: Coronavirus disease 2019 (COVID-19); machine-learning; prediction model; quantitative computed tomography (quantitative CT); respiratory failure.
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1076/coif). The series “Current Status of Diagnosis and Forecast of COVID-19” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous