

Risk Factors Associated With Antimicrobial Resistance and Adverse Short-Term Health Outcomes Among Adult and Adolescent Female Outpatients With Uncomplicated Urinary Tract Infection
- PMID: 37065971
- PMCID: PMC10101691
- DOI: 10.1093/ofid/ofac623
Risk Factors Associated With Antimicrobial Resistance and Adverse Short-Term Health Outcomes Among Adult and Adolescent Female Outpatients With Uncomplicated Urinary Tract Infection
Abstract
Background: Increasing antimicrobial resistance makes treating uncomplicated urinary tract infections (uUTIs) difficult. We compared whether adverse short-term outcomes among US female patients were more common when initial antimicrobial therapy did not cover the causative uropathogen.
Methods: This retrospective cohort study used data from female outpatients aged ≥12 years, with a positive urine culture and dispensing of an oral antibiotic ±1 day from index culture. Isolate susceptibility to the antimicrobial initially dispensed, patient age, and history of antimicrobial exposure, resistance, and all-cause hospitalization within 12 months of index culture were evaluated for associations with adverse outcomes during 28-day follow up. Outcomes assessed were new antimicrobial dispensing, all-cause hospitalization, and all-cause outpatient emergency department/clinic visits.
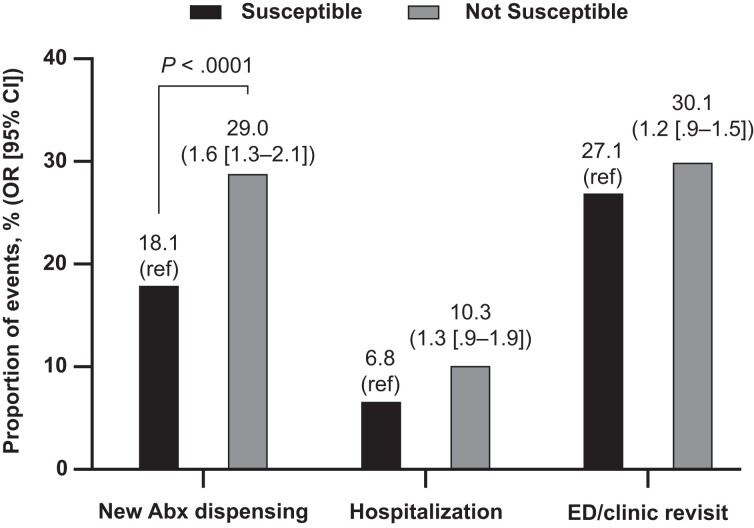
Results: Of 2366 uUTIs, 1908 (80.6%) were caused by isolates susceptible and 458 (19.4%) by isolates not susceptible (intermediate/resistant) to initial antimicrobial treatment. Within 28 days, patients with episodes caused by not susceptible isolates were 60% more likely to receive a new antimicrobial versus episodes with susceptible isolates (29.0% vs 18.1%; 95% confidence interval, 1.3-2.1; P < .0001). Other variables associated with new antibiotic dispenses within 28 days were older age, prior antimicrobial exposure, or prior nitrofurantoin-not-susceptible uropathogens (P < .05). Older age, prior antimicrobial-resistant urine isolates, and prior hospitalization were associated with all-cause hospitalization (P < .05). Prior fluoroquinolone-not-susceptible isolates or oral antibiotic dispensing within 12 months of index culture were associated with subsequent all-cause outpatient visits (P < .05).
Conclusions: New antimicrobial dispensing within the 28-day follow-up period was associated with uUTIs where the uropathogen was not susceptible to initial antimicrobial treatment. Older age and prior antimicrobial exposure, resistance, and hospitalization also identified patients at risk of adverse outcomes.
Keywords: antimicrobial resistance; health outcomes; hospitalization; treatment failure; uncomplicated UTI.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2022.
Conflict of interest statement
Potential conflicts of interest. B. W. T. reports funding from Genentech and INSIGHT (National Institutes of Health National Institute of Allergy and Infectious Diseases) for sponsored trials of potential COVID therapeutics and from VA’s Health Services Research and Development Service ([VA HSR&D] HX002171), VA Rehabilitation Research & Development Service ([RR&D] RX002596), and Agency for Healthcare Research and Quality [AHRQ] (HS026901 and HS027869) for investigator-initiated research. Her work is also funded in part by the Houston Veterans Affairs Health Services Research & Development Center for Innovations in Quality, Effectiveness and Safety (CIN 13-413). The contents of this manuscript do not represent the views of VA or the United States Government. K. S. K. has received symposia honoraria from GSK. V. G. is an employee of and shareholder in Becton, Dickinson and Company, which received funding from GSK to conduct this study. A. M. is an employee and shareholder in GSK. F. S. M.-G. is an employee of and shareholder in GSK. N. E. S.-O. is an employee of and shareholder in GSK. K. Y. is an employee of and shareholder in Becton, Dickinson and Company, which received funding from GSK to conduct this study. G. Y. is an employee of Becton, Dickinson and Company, which received funding from GSK to conduct this study. A. V. J. is an employee of and shareholder in GSK. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Similar articles
-
Economic burden of antibiotic-not-susceptible isolates in uncomplicated urinary tract infection: Analysis of a US integrated delivery network database.Antimicrob Resist Infect Control. 2022 Jun 14;11(1):84. doi: 10.1186/s13756-022-01121-y. Antimicrob Resist Infect Control. 2022. PMID: 35701853 Free PMC article.
-
Impact of suboptimal or inappropriate treatment on healthcare resource use and cost among patients with uncomplicated urinary tract infection: an analysis of integrated delivery network electronic health records.Antimicrob Resist Infect Control. 2022 Nov 4;11(1):133. doi: 10.1186/s13756-022-01170-3. Antimicrob Resist Infect Control. 2022. PMID: 36333740 Free PMC article.
-
Interaction between Antibiotic Resistance, Resistance Genes, and Treatment Response for Urinary Tract Infections in Primary Care.J Clin Microbiol. 2019 Aug 26;57(9):e00143-19. doi: 10.1128/JCM.00143-19. Print 2019 Sep. J Clin Microbiol. 2019. PMID: 31243084 Free PMC article.
-
The current management strategies for community-acquired urinary tract infection.Infect Dis Clin North Am. 2003 Jun;17(2):303-32. doi: 10.1016/s0891-5520(03)00004-7. Infect Dis Clin North Am. 2003. PMID: 12848472 Review.
-
Sulopenem: An Intravenous and Oral Penem for the Treatment of Urinary Tract Infections Due to Multidrug-Resistant Bacteria.Drugs. 2022 Apr;82(5):533-557. doi: 10.1007/s40265-022-01688-1. Epub 2022 Mar 16. Drugs. 2022. PMID: 35294769 Review.
Cited by
-
Risk Factors for Empiric Treatment Failure in US Female Outpatients with Uncomplicated Urinary Tract Infection: an Observational Study.J Gen Intern Med. 2025 Mar;40(4):862-870. doi: 10.1007/s11606-024-09029-6. Epub 2024 Oct 2. J Gen Intern Med. 2025. PMID: 39356448 Free PMC article.
-
Living With and Managing Uncomplicated Urinary Tract Infection: Mixed Methods Analysis of Patient Insights From Social Media.J Med Internet Res. 2025 Mar 11;27:e58882. doi: 10.2196/58882. J Med Internet Res. 2025. PMID: 40067345 Free PMC article.
-
Impact of empirical treatment failure on health care resource utilization and costs among female patients with uncomplicated urinary tract infections in a US-based Integrated Health Delivery Network.J Manag Care Spec Pharm. 2025 Sep;31(9):879-889. doi: 10.18553/jmcp.2025.31.9.879. J Manag Care Spec Pharm. 2025. PMID: 40884226 Free PMC article.
-
Co-resistance Among Escherichia coli and Klebsiella pneumoniae Urine Isolates from Female Outpatients with Presumed UTI: A Retrospective US Cohort Study.Infect Dis Ther. 2024 Jul;13(7):1715-1722. doi: 10.1007/s40121-024-00995-2. Epub 2024 Jun 6. Infect Dis Ther. 2024. PMID: 38842759 Free PMC article.
-
Prevalence, regional distribution, and trends of antimicrobial resistance among female outpatients with urine Klebsiella spp. isolates: a multicenter evaluation in the United States between 2011 and 2019.Antimicrob Resist Infect Control. 2024 Feb 14;13(1):21. doi: 10.1186/s13756-024-01372-x. Antimicrob Resist Infect Control. 2024. PMID: 38355621 Free PMC article.
