

Respiratory Syncytial Virus Disease Burden in Community-Dwelling and Long-Term Care Facility Older Adults in Europe and the United States: A Prospective Study
- PMID: 37065988
- PMCID: PMC10099469
- DOI: 10.1093/ofid/ofad111
Respiratory Syncytial Virus Disease Burden in Community-Dwelling and Long-Term Care Facility Older Adults in Europe and the United States: A Prospective Study
Abstract
Background: Data on respiratory syncytial virus (RSV) disease burden in adults remain scarce. We assessed the burden of confirmed RSV-acute respiratory infections (cRSV-ARIs) in community-dwelling (CD) adults and those in long-term care facilities (LTCFs).
Methods: In this prospective cohort study covering 2 RSV seasons (October 2019-March 2020 and October 2020-June 2021), RSV-ARIs were identified through active surveillance, in medically stable CD-adults ≥50 years (Europe) or adults ≥65 years in LTCFs (Europe and the United States). RSV infection was confirmed by polymerase chain reaction from combined nasal and throat swabs.
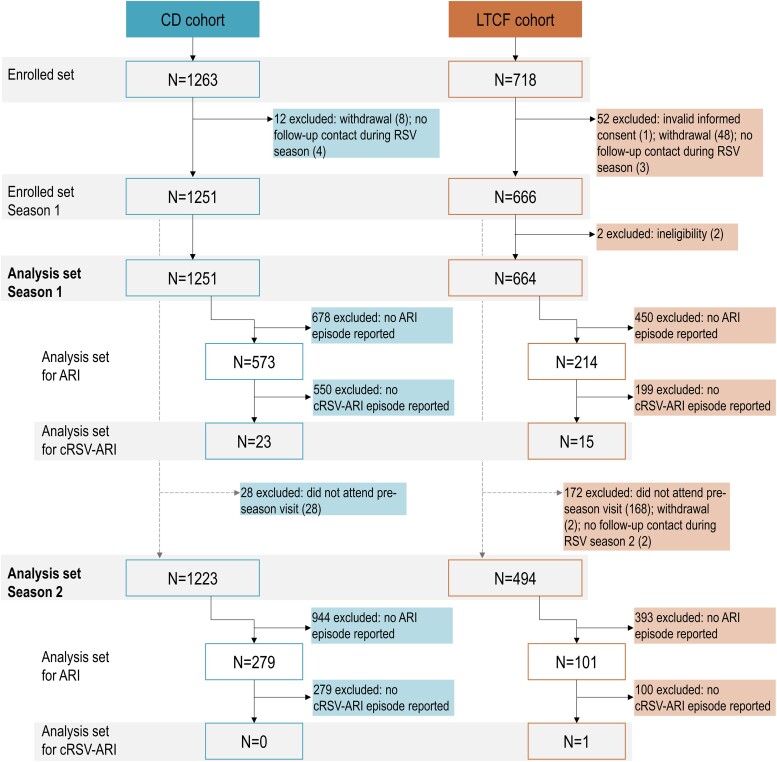
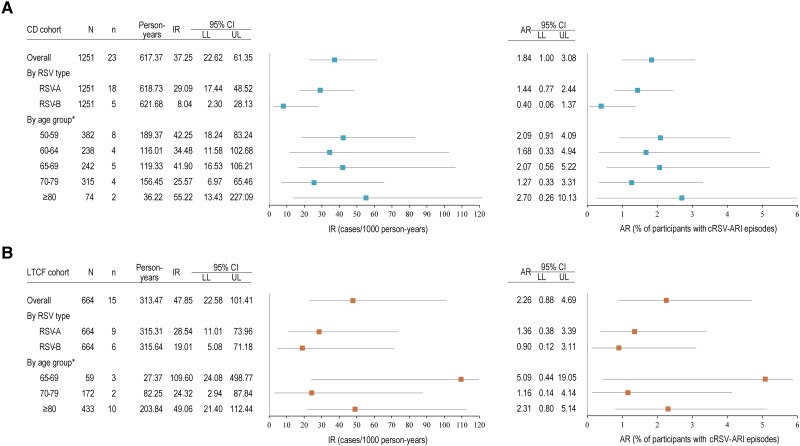
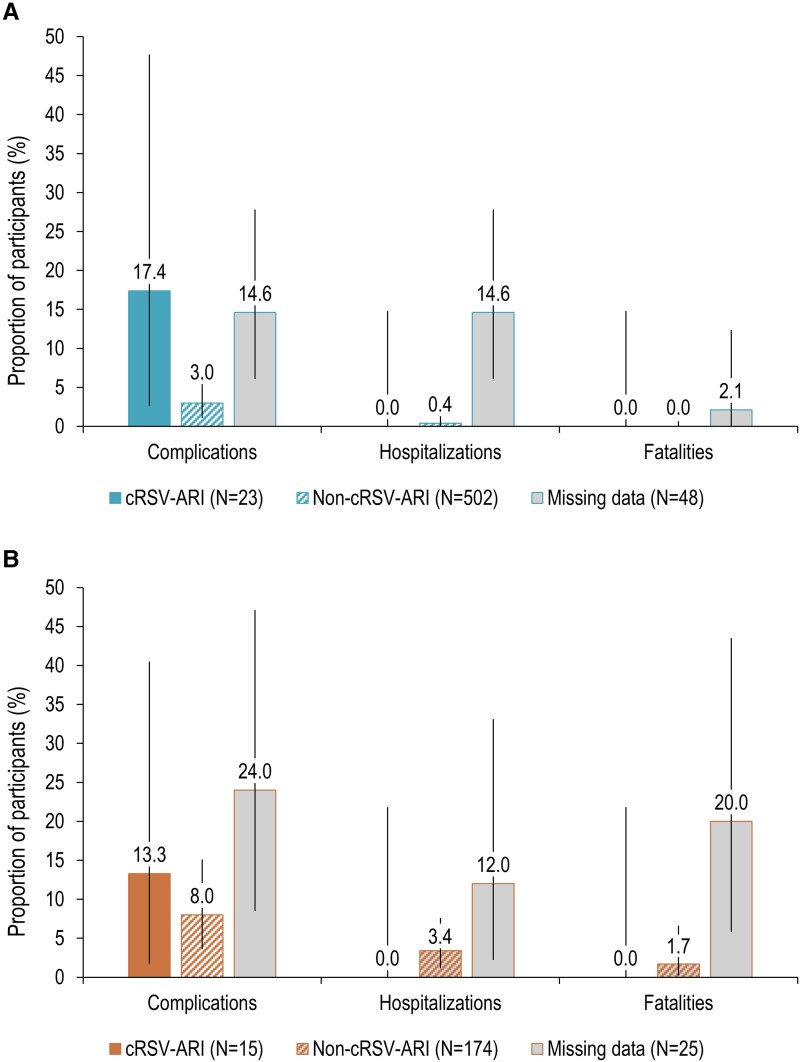
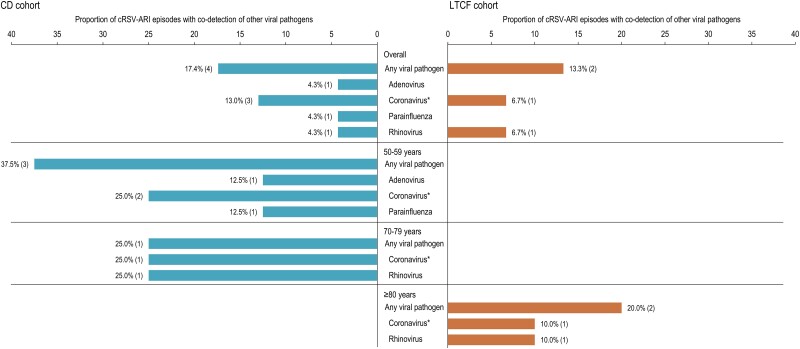
Results: Of 1981 adults enrolled, 1251 adults in CD and 664 LTCFs (season 1) and 1223 adults in CD and 494 LTCFs (season 2) were included in the analyses. During season 1, overall incidence rates ([IRs] cases/1000 person-years) and attack rates (ARs) for cRSV-ARIs were 37.25 (95% confidence interval [CI], 22.62-61.35) and 1.84% in adults in CD and 47.85 (CI, 22.58-101.4) and 2.26% in adults in LTCFs. Complications occurred for 17.4% (CD) and 13.3% (LTCFs) of cRSV-ARIs. One cRSV-ARI occurred in season 2 (IR = 2.91 [CI, 0.40-20.97]; AR = 0.20%), without complications. No cRSV-ARIs led to hospitalization or death. Viral pathogens were codetected in ≤17.4% of cRSV-ARIs.
Conclusions: RSV is an important cause of disease burden in adults in CD and LTCFs. Despite the observed low severity of cRSV-ARI, our results support the need for RSV prevention strategies among adults ≥50 years old.
Keywords: care facilities; community-dwelling; incidence/burden of disease; older adults; respiratory syncytial virus infection.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. RD, SD, J-YP, and DL are employees of the GSK group of companies. SD, J-YP, and DL hold shares in the GSK group of companies as part of their employee remuneration. JMRT declares lectures for Pfizer and attending meetings for GSK and Pfizer. IL-R declares funding from GSK, ICOSAVAX, and Virometix to her institution for conducting RSV clinical trials and participation on Janssen advisory boards for RSV vaccines. CV reports grant/research support from GSK to her institution for the conduct of the current study and is currently an employee of the GSK group of companies. KS, JSTB, and LLH declares research funding received by their institution from GSK. RGF declares lectures for GSK. SM works as a freelance consultant on behalf of the GSK group of companies. All other authors declare no conflict of interest.
Figures
References
-
- Coates HV, Alling DW, Chanock RM. An antigenic analysis of respiratory syncytial virus isolates by a plaque reduction neutralization test. Am J Epidemiol 1966; 83:299–313. - PubMed
-
- Walsh EE, Falsey AR. Respiratory syncytial virus infection in adult populations. Infect Disord Drug Targets 2012; 12:98–102. - PubMed
-
- Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med 2005; 352:1749–59. - PubMed
