

Management of acute aortic syndrome with evolving individualized precision medicine solutions: Lessons learned over two decades and literature review
- PMID: 37065997
- PMCID: PMC10097442
- DOI: 10.3389/fsurg.2023.1157457
Management of acute aortic syndrome with evolving individualized precision medicine solutions: Lessons learned over two decades and literature review
Abstract
Background: Thoracoabdominal acute aortic syndrome is associated with high morbidity and mortality. We aim to scrutinize our evolving strategies for acute aortic syndrome (AAS) management using minimally invasive and adaptive surgical techniques over two decades.
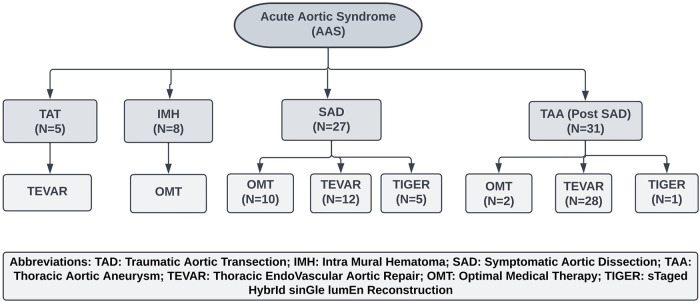
Methods: This is a longitudinal observational study at our tertiary vascular centre from 2002 to 2021. Out of 22,349 aortic referrals, we performed 1,555 aortic interventions over twenty years. Amongst 96 presented with symptomatic aortic thoracic pathology, 71 patients had AAS. Our primary endpoint is combined aneurysm-related and cardiovascular-related mortality.
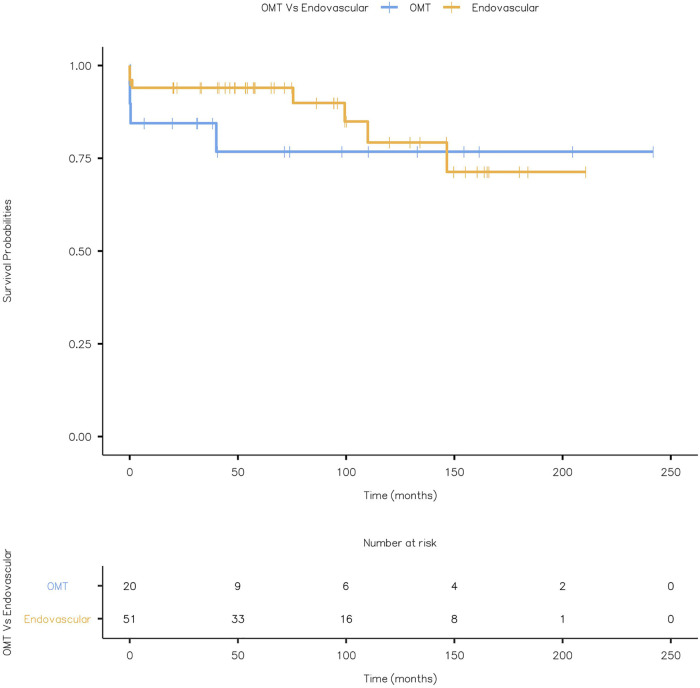
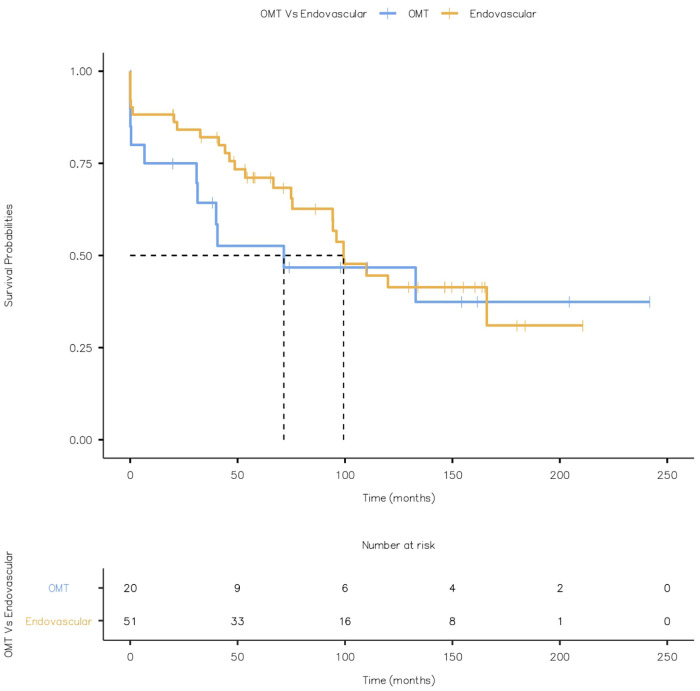
Results: There were 43 males and 28 females (5 Traumatic Aortic Transection (TAT), 8 Acute Aortic Intramural Hematoma (IMH), 27 Symptomatic Aortic Dissection (SAD) and 31 Thoracic Aortic Aneurysm (TAA) post-SAD) with a mean age of 69. All the patients with AAS received optimal medical therapy (OMT), but TAT patients underwent emergency thoracic endovascular aortic repair (TEVAR). Fifty-eight patients had an aortic dissection, of which 31 developed TAA. These 31 patients with SAD and TAA received OMT initially and interval surgical intervention with TEVAR or sTaged hybrId sinGle lumEn Reconstruction (TIGER). To increase our landing area, we performed a left subclavian chimney graft with TEVAR in twelve patients. The average follow-up duration was 78.2 months, and eleven patients (15.5%) had combined aneurysm and cardiovascular-related mortality. Twenty-six percentage of the patients developed endoleaks (EL), of which 15% required re-intervention for type II and III. Four patients who had paraplegia (5.7%) and developed renal failure died. None of our patients had a stroke or bowel ischaemia. Twenty patients had OMT, eight of these were patients with acute aortic hematoma, and all eight died within 30 days of presentation.
Conclusion: Acute aortic hematoma is a sinister finding, which must be closely monitored, and consideration is given to early intervention. Paraplegia and renal failure result in an increased mortality rate. TIGER technique with interval TEVAR has salvaged complex situations in young patients. Left subclavian chimney increases our landing area and abolishes SINE. Our experience shows that minimally invasive techniques could be a viable option for AAS.
Keywords: acute aortic syndrome (AAS); hybrid endovascular repair; stent-graft induced new entry tear (SINE); thoracic endovascular aneurysm repair (TEVAR); thoraco-abdominal aorta.
© 2023 Sultan, Acharya, Chua Vi Long, Hatem, Hezima, Veerasingham, Soliman and Hynes.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
In situ laser fenestration during emergent thoracic endovascular aortic repair is an effective method for left subclavian artery revascularization.J Vasc Surg. 2013 Nov;58(5):1171-7. doi: 10.1016/j.jvs.2013.04.045. Epub 2013 Jun 5. J Vasc Surg. 2013. PMID: 23746832
-
When is extra-anatomical bypass for the left subclavian artery required to prevent ischaemia after thoracic endovascular stent grafting?Asian Cardiovasc Thorac Ann. 2021 Jul;29(6):524-531. doi: 10.1177/02184923211008074. Epub 2021 Apr 4. Asian Cardiovasc Thorac Ann. 2021. PMID: 33818153
-
Single-center experience with simultaneous thoracic endovascular aortic repair and abdominal endovascular aneurysm repair.Vascular. 2017 Apr;25(2):157-162. doi: 10.1177/1708538116651020. Epub 2016 Jul 9. Vascular. 2017. PMID: 27334106
-
Comparison of the efficacy and safety of thoracic endovascular aortic repair with open surgical repair and optimal medical therapy for acute type B aortic dissection: A systematic review and meta-analysis.Int J Surg. 2020 Nov;83:53-61. doi: 10.1016/j.ijsu.2020.08.051. Epub 2020 Sep 11. Int J Surg. 2020. PMID: 32927144
-
Medical and surgical management of acute type B aortic intramural hematoma.J Card Surg. 2020 Sep;35(9):2324-2330. doi: 10.1111/jocs.14823. Epub 2020 Jul 15. J Card Surg. 2020. PMID: 32668075 Review.
Cited by
-
Mechanisms of aortic dissection: From pathological changes to experimental and in silico models.Prog Mater Sci. 2025 Apr;150:101363. doi: 10.1016/j.pmatsci.2024.101363. Epub 2024 Sep 12. Prog Mater Sci. 2025. PMID: 39830801 Free PMC article.
-
Acute aortic catastrophe caused by cardiovascular oncological manipulation by tyrosine kinase inhibitors with immune checkpoint blockades: a case report and literature review.Eur Heart J Case Rep. 2024 Apr 5;8(4):ytae169. doi: 10.1093/ehjcr/ytae169. eCollection 2024 Apr. Eur Heart J Case Rep. 2024. PMID: 38887778 Free PMC article.
-
Systematic review of cardiovascular neurocristopathy-contemporary insights and future perspectives.Front Cardiovasc Med. 2024 Apr 9;11:1333265. doi: 10.3389/fcvm.2024.1333265. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38660479 Free PMC article.
References
-
- Coselli JS, de Figueiredo LF. Natural history of descending and thoracoabdominal aortic aneurysms. J Card Surg. (1997) 12(2 Suppl):285–91. - PubMed
-
- Suzuki T, Mehta RH, Ince H, Nagai R, Sakomura Y, Weber F, et al. Clinical profiles and outcomes of acute type B aortic dissection in the current era: lessons from the international registry of aortic dissection (IRAD). Circulation. (2003) 108(Suppl 1):II312–7. 10.1161/01.cir.0000087386.07204.09 - DOI - PubMed
-
- Bickerstaff LK, Pairolero PC, Hollier LH, Melton LJ, Van Peenen HJ, Cherry KJ, et al. Thoracic aortic aneurysms: a population-based study. Surgery. (1982) 92(6):1103–8. - PubMed
LinkOut - more resources
Full Text Sources