

Opportunities for Achieving the Cancer Moonshot Goal of a 50% Reduction in Cancer Mortality by 2047
- PMID: 37067240
- PMCID: PMC10164123
- DOI: 10.1158/2159-8290.CD-23-0208
Opportunities for Achieving the Cancer Moonshot Goal of a 50% Reduction in Cancer Mortality by 2047
Abstract
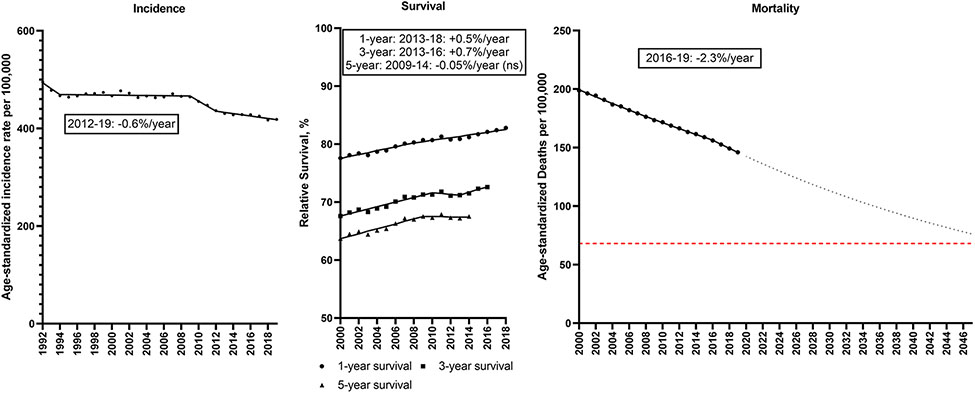
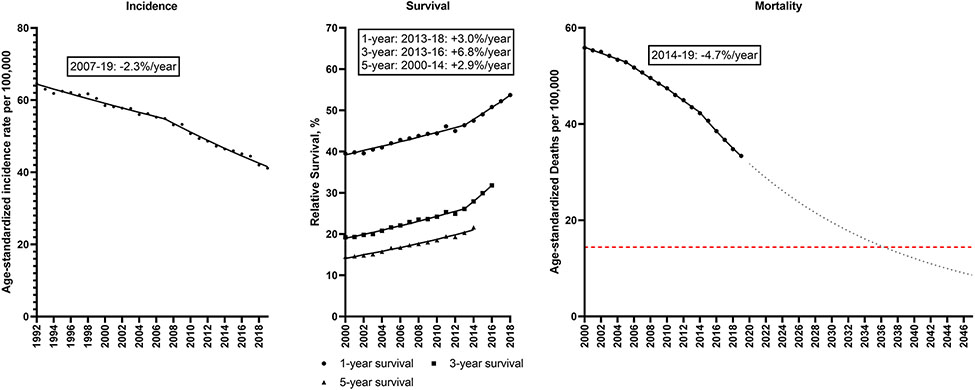
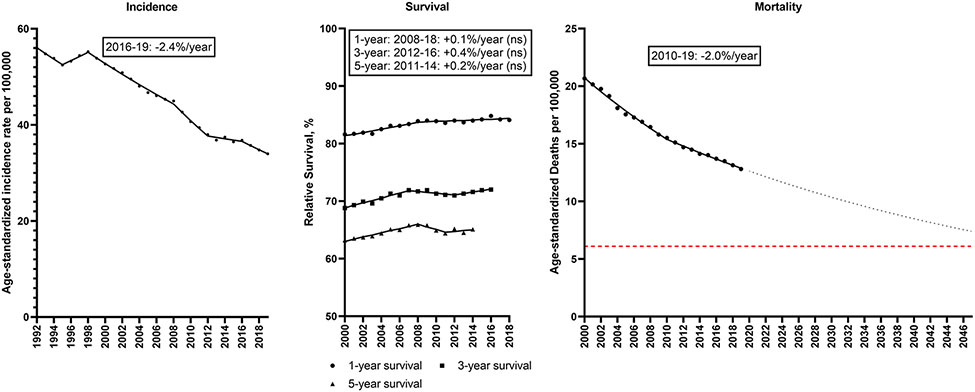
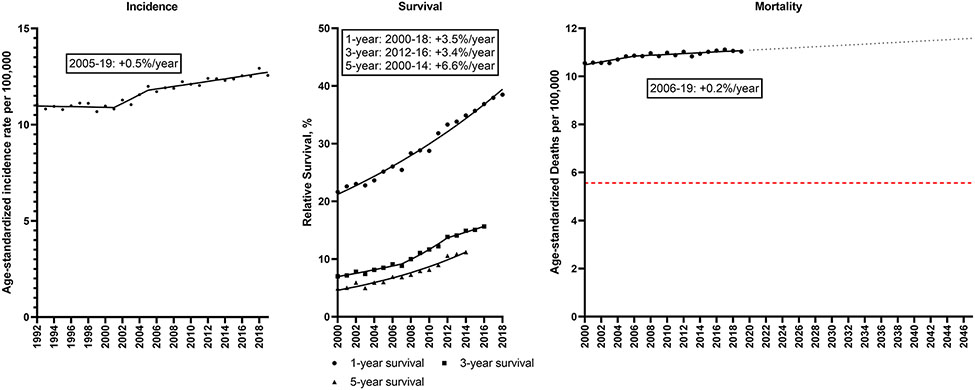
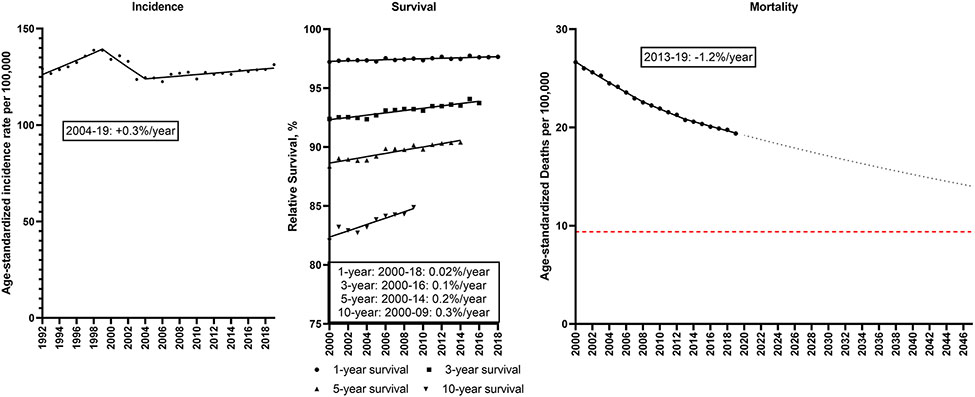
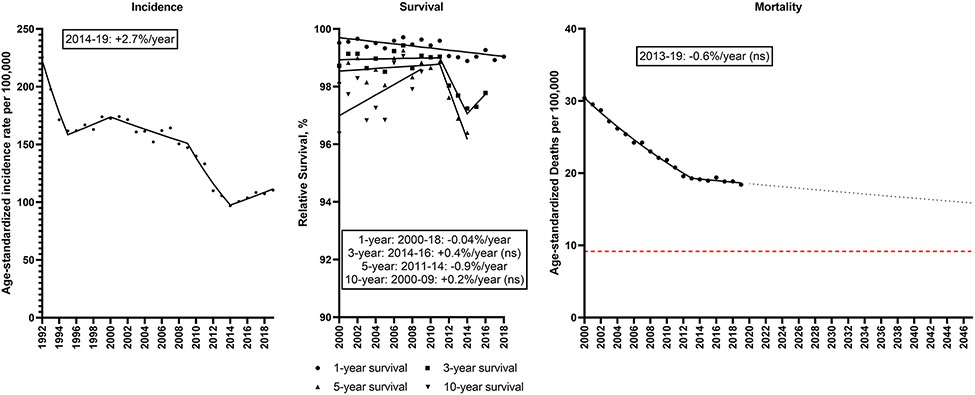
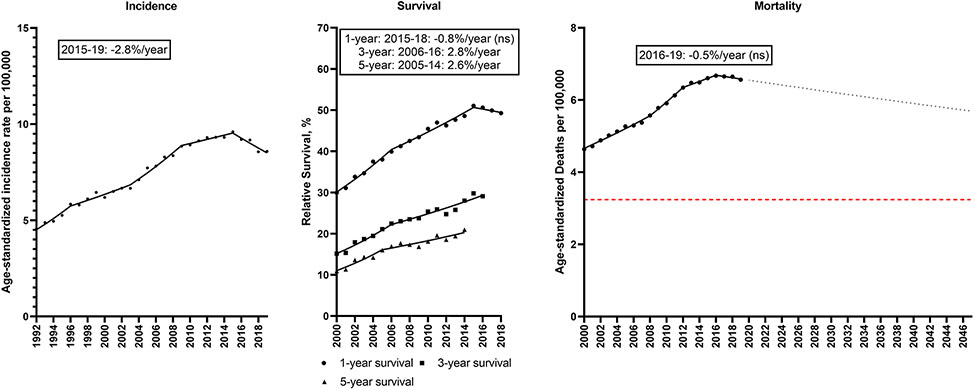
On February 2, 2022, President Biden and First Lady Dr. Biden reignited the Cancer Moonshot, setting a new goal to reduce age-standardized cancer mortality rates by at least 50% over the next 25 years in the United States. We estimated trends in U.S. cancer mortality during 2000 to 2019 for all cancers and the six leading types (lung, colorectum, pancreas, breast, prostate, liver). Cancer death rates overall declined by 1.4% per year from 2000 to 2015, accelerating to 2.3% per year during 2016 to 2019, driven by strong declines in lung cancer mortality (-4.7%/year, 2014 to 2019). Recent declines in colorectal (-2.0%/year, 2010-2019) and breast cancer death rates (-1.2%/year, 2013-2019) also contributed. However, trends for other cancer types were less promising. To achieve the Moonshot goal, progress against lung, colorectal, and breast cancer deaths needs to be maintained and/or accelerated, and new strategies for prostate, liver, pancreatic, and other cancers are needed. We reviewed opportunities to prevent, detect, and treat these common cancers that could further reduce population-level cancer death rates and also reduce disparities.
Significance: We reviewed opportunities to prevent, detect, and treat common cancers, and show that to achieve the Moonshot goal, progress against lung, colorectal, and breast cancer deaths needs to be maintained and/or accelerated, and new strategies for prostate, liver, pancreatic, and other cancers are needed. See related commentary by Bertagnolli et al., p. 1049. This article is highlighted in the In This Issue feature, p. 1027.
©2023 American Association for Cancer Research.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
Achieving the Goals of the Cancer Moonshot Requires Progress against All Cancers.Cancer Discov. 2023 May 4;13(5):1049-1052. doi: 10.1158/2159-8290.CD-23-0344. Cancer Discov. 2023. PMID: 37067233
Comment on
-
Achieving the Goals of the Cancer Moonshot Requires Progress against All Cancers.Cancer Discov. 2023 May 4;13(5):1049-1052. doi: 10.1158/2159-8290.CD-23-0344. Cancer Discov. 2023. PMID: 37067233
References
-
- Xu J, Murphy S, Kochenek K, Arias E. Deaths: Final Deata for 2019. National Vital Statistics Reports 2021;70(8). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
