

Serum procalcitonin level is independently associated with mechanical ventilation and case-fatality in hospitalized COVID-19-positive US veterans-A potential marker for disease severity
- PMID: 37068086
- PMCID: PMC10109491
- DOI: 10.1371/journal.pone.0284520
Serum procalcitonin level is independently associated with mechanical ventilation and case-fatality in hospitalized COVID-19-positive US veterans-A potential marker for disease severity
Abstract
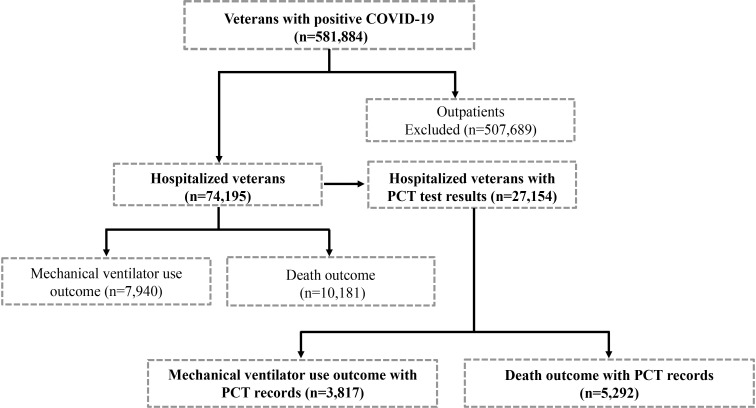
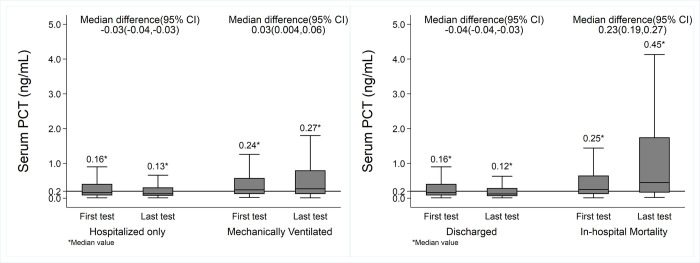
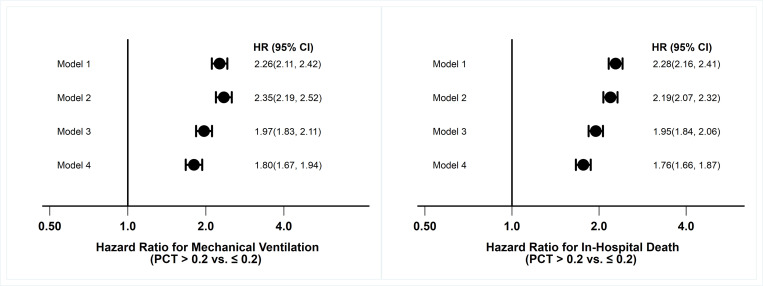
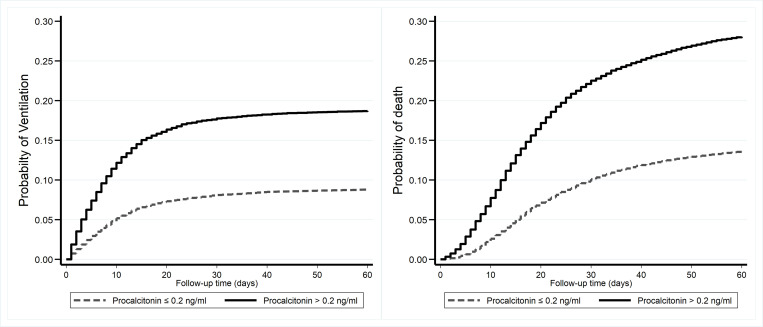
The Coronavirus-19 disease (COVID-19) has claimed over 6.8 million lives since first being reported in late 2019. The virus that causes COVID-19 disease is highly contagious and spreads rapidly. To date, there are no approved prognostic tools that could predict why some patients develop severe or fatal disease outcomes. Early COVID-19 studies found an association between procalcitonin (PCT) and hospitalization or duration of mechanical ventilation and death but were limited by the cohort sizes. Therefore, this study was designed to confirm the associations of PCT with COVID-19 disease severity outcomes in a large cohort. For this retrospective data analysis study, 27,154 COVID-19-positive US veterans with post-infection PCT laboratory test data and their disease severity outcomes were accessed using the VA electronic healthcare data. Cox regression models were used to test the association between serum PCT levels and disease outcomes while controlling for demographics and relevant confounding variables. The models demonstrated increasing disease severity (ventilation and death) with increasing PCT levels. For PCT serum levels above 0.20 ng/ml, the unadjusted risk increased nearly 2.3-fold for mechanical ventilation (hazard ratio, HR, 2.26, 95%CI: 2.11-2.42) and in-hospital death (HR, 2.28, 95%CI: 2.16-2.41). Even when adjusted for demographics, diabetes, pneumonia, antibiotic use, white blood cell count, and serum C-reactive protein levels, the risks remained relatively high for mechanical ventilation (HR, 1.80, 95%CI: 1.67-1.94) and death (HR, 1.76, 95%CI: 1.66-1.87). These data suggest that higher PCT levels have independent associations with ventilation and in-hospital death in veterans with COVID-19 disease, validating previous findings. The data suggested that serum PCT level may be a promising prognostic tool for COVID-19 severity assessment and should be further evaluated in a prospective clinical trial.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The role of procalcitonin in predicting risk of mechanical ventilation and mortality among moderate to severe COVID-19 patients.BMC Infect Dis. 2022 Apr 15;22(1):378. doi: 10.1186/s12879-022-07362-x. BMC Infect Dis. 2022. PMID: 35428273 Free PMC article.
-
Association of procalcitonin levels with the progression and prognosis of hospitalized patients with COVID-19.Int J Med Sci. 2020 Sep 9;17(16):2468-2476. doi: 10.7150/ijms.48396. eCollection 2020. Int J Med Sci. 2020. PMID: 33029089 Free PMC article.
-
Searching for a role of procalcitonin determination in COVID-19: a study on a selected cohort of hospitalized patients.Clin Chem Lab Med. 2020 Nov 19;59(2):433-440. doi: 10.1515/cclm-2020-1361. Clin Chem Lab Med. 2020. PMID: 33554505
-
The Level of Procalcitonin in Severe COVID-19 Patients: A Systematic Review and Meta-Analysis.Adv Exp Med Biol. 2021;1321:277-286. doi: 10.1007/978-3-030-59261-5_25. Adv Exp Med Biol. 2021. PMID: 33656733
-
The efficacy of procalcitonin as a biomarker in the management of sepsis: slaying dragons or tilting at windmills?Surg Infect (Larchmt). 2013 Dec;14(6):489-511. doi: 10.1089/sur.2012.028. Epub 2013 Nov 25. Surg Infect (Larchmt). 2013. PMID: 24274059 Review.
Cited by
-
Development and validation of a prognostic model based on clinical laboratory biomarkers to predict admission to ICU in Omicron variant-infected hospitalized patients complicated with myocardial injury.Front Immunol. 2024 Feb 1;15:1268213. doi: 10.3389/fimmu.2024.1268213. eCollection 2024. Front Immunol. 2024. PMID: 38361939 Free PMC article. Clinical Trial.
-
Role of Procalcitonin as a Prognostic Biomarker in Hospitalized COVID-19 Patients: A Comparative Analysis.Biomark Insights. 2025 May 15;20:11772719241296624. doi: 10.1177/11772719241296624. eCollection 2025. Biomark Insights. 2025. PMID: 40386243 Free PMC article.
-
A retrospective propensity-score-matched cohort study of the impact of procalcitonin testing on antibiotic use in hospitalized patients during the first wave of COVID-19.J Antimicrob Chemother. 2024 Nov 4;79(11):2792-2800. doi: 10.1093/jac/dkae246. J Antimicrob Chemother. 2024. PMID: 39248146 Free PMC article.
-
Utility of Serum Procalcitonin and Its Clearance in Predicting Outcomes in COVID-19 Patients.Cureus. 2024 May 13;16(5):e60203. doi: 10.7759/cureus.60203. eCollection 2024 May. Cureus. 2024. PMID: 38868239 Free PMC article.
References
-
- WHO. WHO Coronavirus (COVID-19) Dashboard 2023. [cited 2023 March 8]. Available from: https://covid19.who.int/.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
