

Unloading the Left Ventricle in Venoarterial ECMO: In Whom, When, and How?
- PMID: 37068133
- PMCID: PMC10217772
- DOI: 10.1161/CIRCULATIONAHA.122.062371
Unloading the Left Ventricle in Venoarterial ECMO: In Whom, When, and How?
Abstract
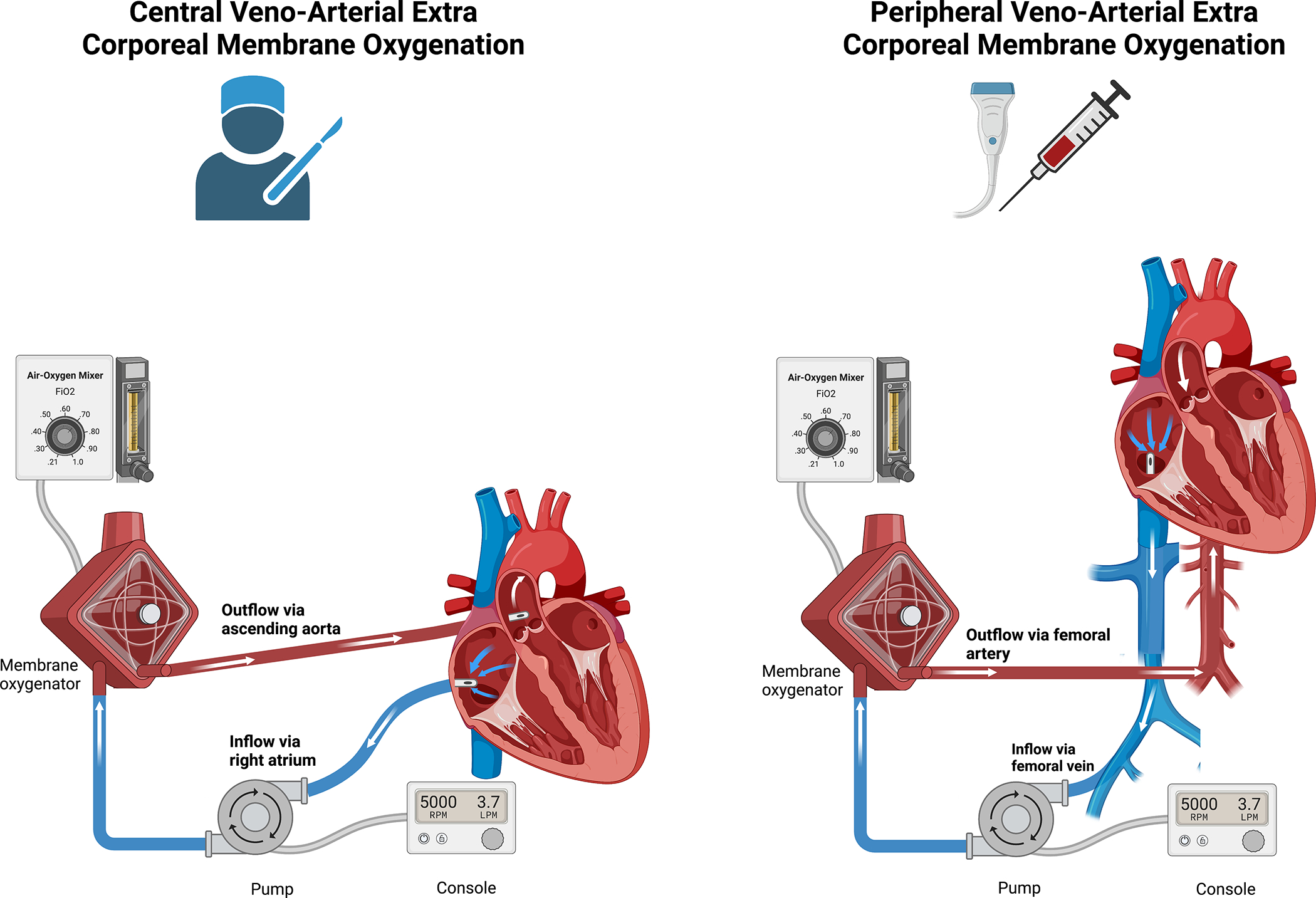
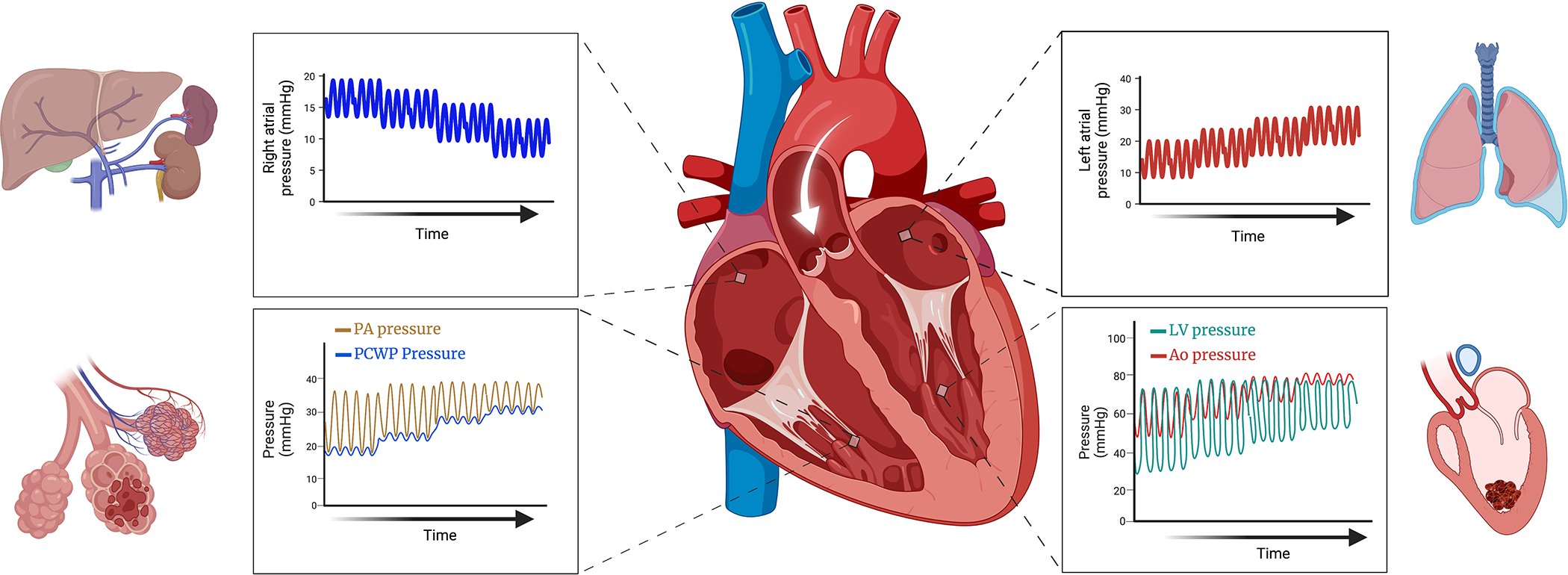
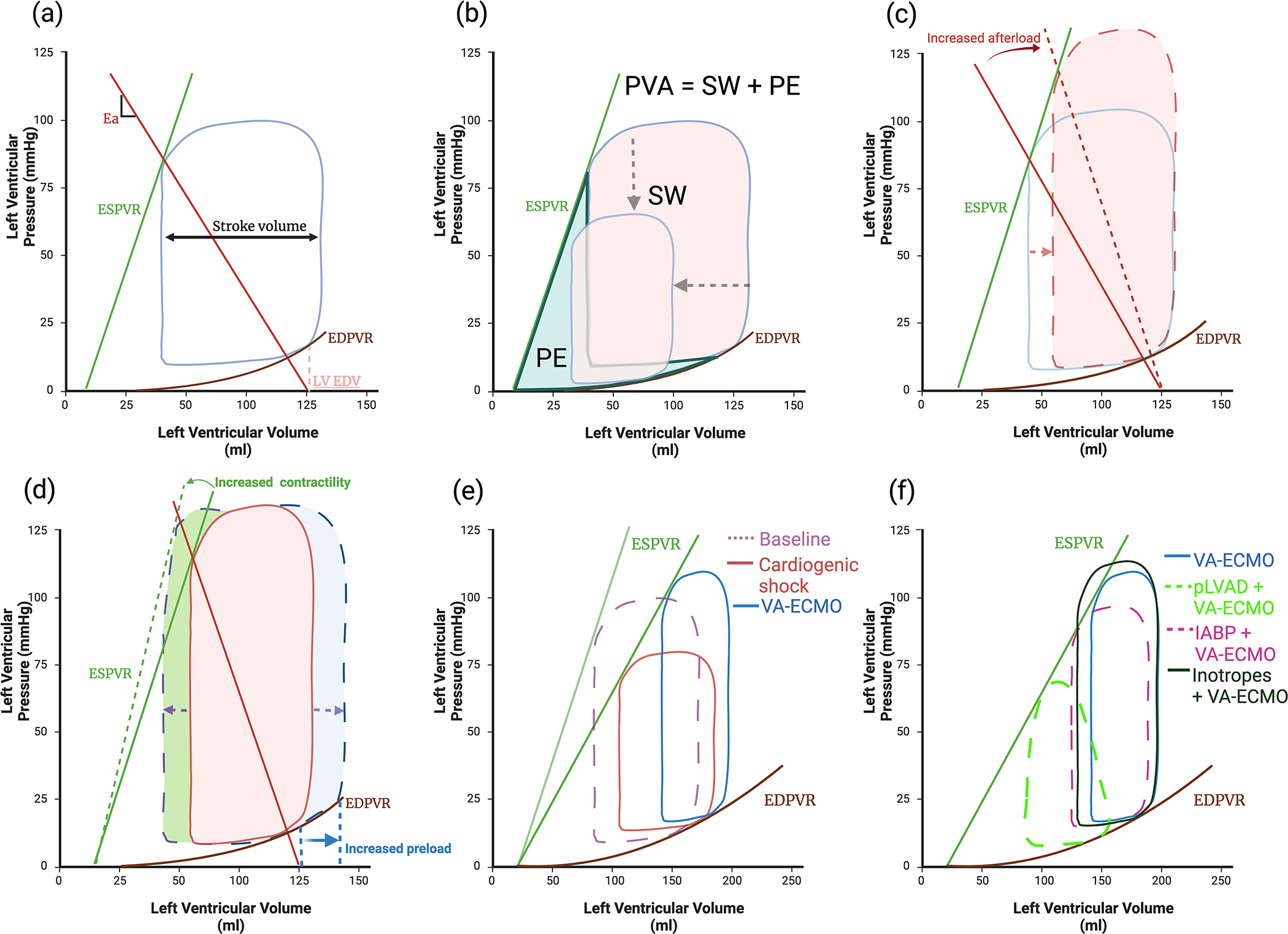
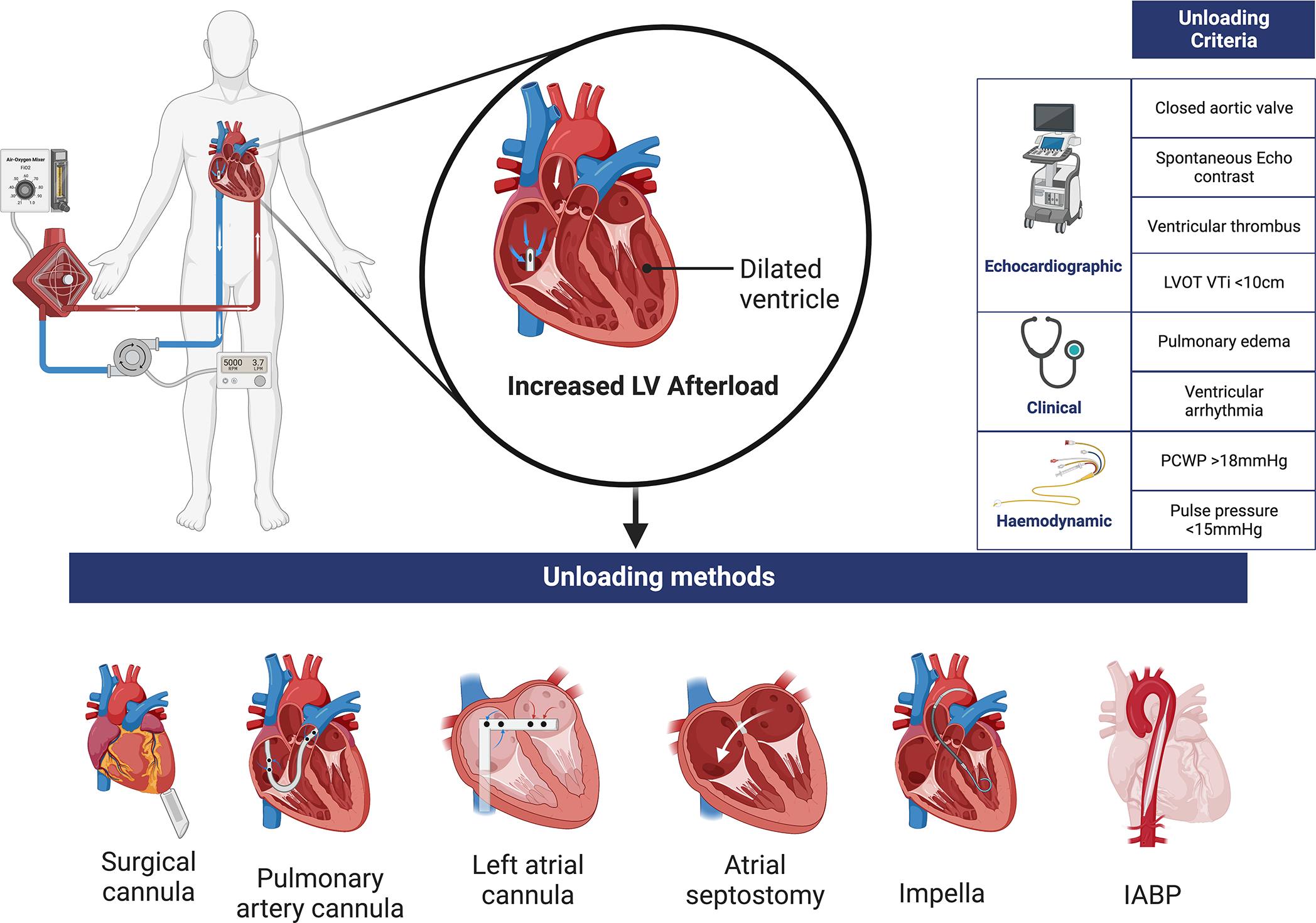
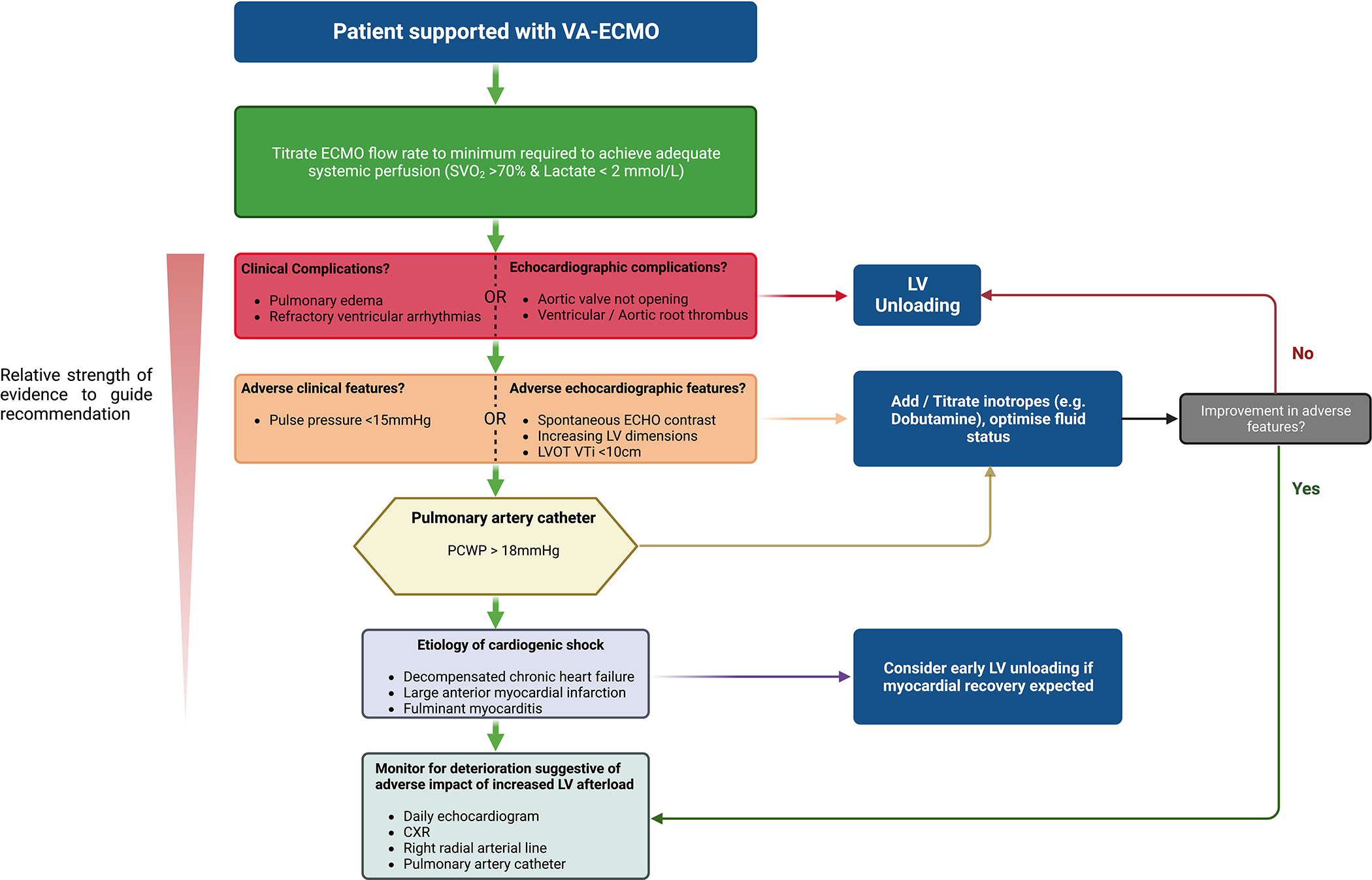
Venoarterial extracorporeal membrane oxygenation provides cardiorespiratory support to patients in cardiogenic shock. This comes at the cost of increased left ventricle (LV) afterload that can be partly ascribed to retrograde aortic flow, causing LV distension, and leads to complications including cardiac thrombi, arrhythmias, and pulmonary edema. LV unloading can be achieved by using an additional circulatory support device to mitigate the adverse effects of mechanical overload that may increase the likelihood of myocardial recovery. Observational data suggest that these strategies may improve outcomes, but in whom, when, and how LV unloading should be employed is unclear; all techniques require balancing presumed benefits against known risks of device-related complications. This review summarizes the current evidence related to LV unloading with venoarterial extracorporeal membrane oxygenation.
Keywords: extracorporeal membrane oxygenation; heart failure; heart-assist devices; hemodynamics; myocardial infarction; shock; shock, cardiogenic.
Figures
References
-
- van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2017;136:e232–e268. doi: 10.1161/CIR.0000000000000525 - DOI - PubMed
-
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999;341:625–634. doi: 10.1056/NEJM199908263410901 - DOI - PubMed
-
- Boulate D, Luyt CE, Pozzi M, Niculescu M, Combes A, Leprince P, Kirsch M. Acute lung injury after mechanical circulatory support implantation in patients on extracorporeal life support: an unrecognized problem. Eur J Cardiothorac Surg. 2013;44:544–549; discussion 549–550. doi: 10.1093/ejcts/ezt125 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
