

Comutations and KRASG12C Inhibitor Efficacy in Advanced NSCLC
- PMID: 37068173
- PMCID: PMC11024958
- DOI: 10.1158/2159-8290.CD-22-1420
Comutations and KRASG12C Inhibitor Efficacy in Advanced NSCLC
Abstract
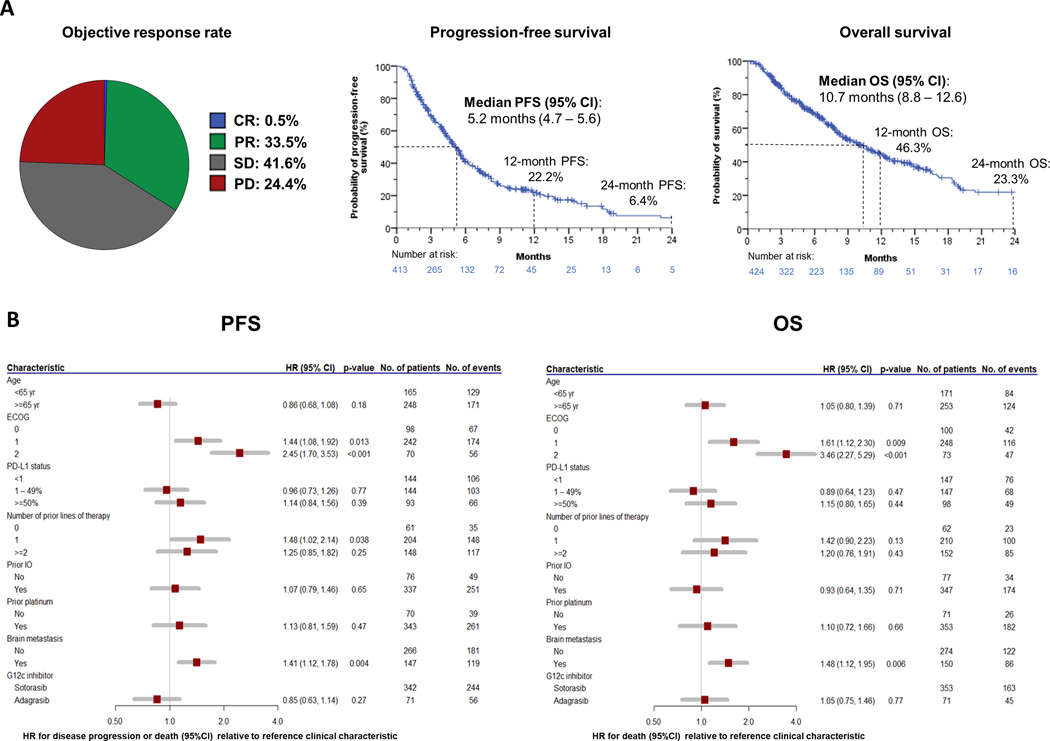
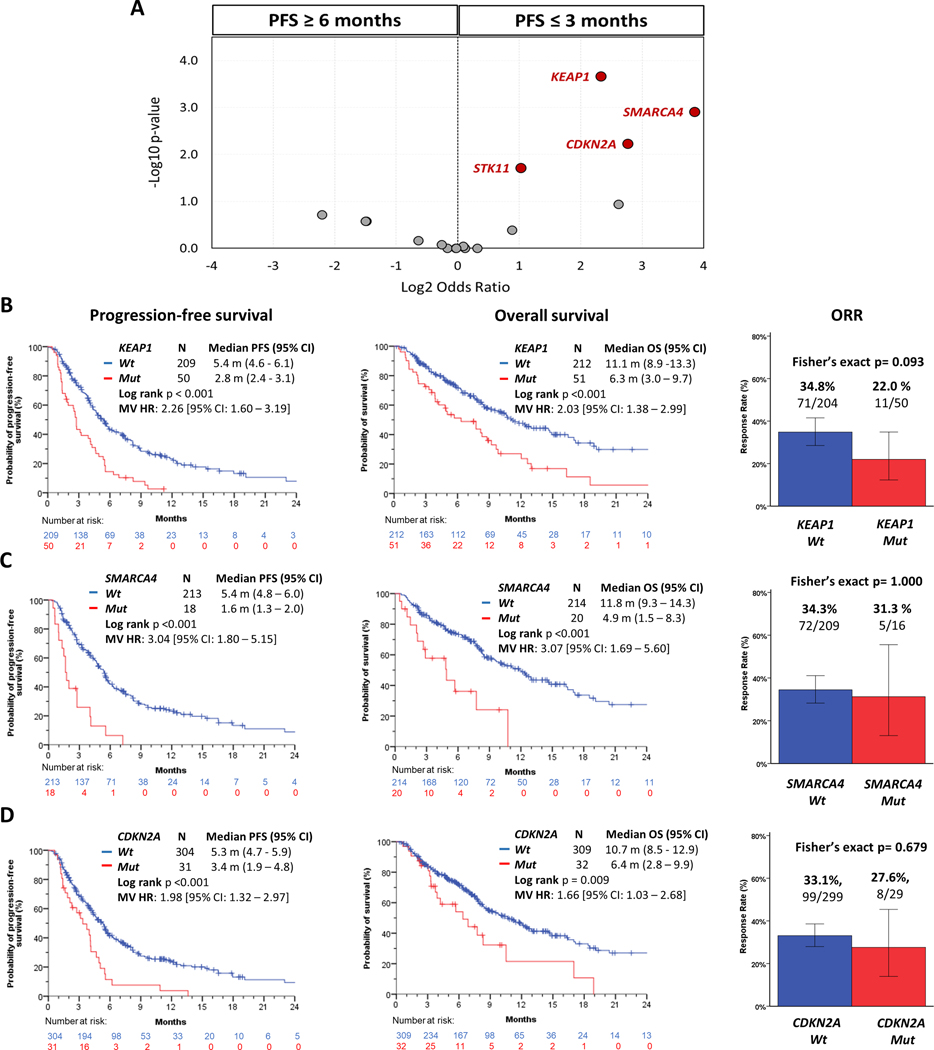
Molecular modifiers of KRASG12C inhibitor (KRASG12Ci) efficacy in advanced KRASG12C-mutant NSCLC are poorly defined. In a large unbiased clinicogenomic analysis of 424 patients with non-small cell lung cancer (NSCLC), we identified and validated coalterations in KEAP1, SMARCA4, and CDKN2A as major independent determinants of inferior clinical outcomes with KRASG12Ci monotherapy. Collectively, comutations in these three tumor suppressor genes segregated patients into distinct prognostic subgroups and captured ∼50% of those with early disease progression (progression-free survival ≤3 months) with KRASG12Ci. Pathway-level integration of less prevalent coalterations in functionally related genes nominated PI3K/AKT/MTOR pathway and additional baseline RAS gene alterations, including amplifications, as candidate drivers of inferior outcomes with KRASG12Ci, and revealed a possible association between defective DNA damage response/repair and improved KRASG12Ci efficacy. Our findings propose a framework for patient stratification and clinical outcome prediction in KRASG12C-mutant NSCLC that can inform rational selection and appropriate tailoring of emerging combination therapies.
Significance: In this work, we identify co-occurring genomic alterations in KEAP1, SMARCA4, and CDKN2A as independent determinants of poor clinical outcomes with KRASG12Ci monotherapy in advanced NSCLC, and we propose a framework for patient stratification and treatment personalization based on the comutational status of individual tumors. See related commentary by Heng et al., p. 1513. This article is highlighted in the In This Issue feature, p. 1501.
©2023 American Association for Cancer Research.
Figures




Comment in
-
Coexisting Genomic Alterations in Risk Stratification of KRASG12C-Mutated Non-Small Cell Lung Cancer.Cancer Discov. 2023 Jul 7;13(7):1513-1515. doi: 10.1158/2159-8290.CD-23-0489. Cancer Discov. 2023. PMID: 37416990
References
-
- Gimple RC, Wang X. RAS: Striking at the Core of the Oncogenic Circuitry [Internet]. Front Oncol. 2019;9:1–16. Available from: https://www.frontiersin.org/article/10.3389/fonc.2019.00965 - DOI - PMC - PubMed
-
- Canon J, Rex K, Saiki AY, Mohr C, Cooke K, Bagal D, et al. The clinical KRAS(G12C) inhibitor AMG 510 drives anti-tumour immunity. Nature. 2019;575:217–23. - PubMed
-
- Hallin J, Engstrom LD, Hargis L, Calinisan A, Aranda R, Briere DM, et al. The KRAS G12C Inhibitor MRTX849 Provides Insight toward Therapeutic Susceptibility of KRAS-Mutant Cancers in Mouse Models and Patients. Cancer Discov [Internet]. 2020;10:54 LP–71. Available from: http://cancerdiscovery.aacrjournals.org/content/10/1/54.abstract - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
