

Circulating proteins to predict COVID-19 severity
- PMID: 37069249
- PMCID: PMC10107586
- DOI: 10.1038/s41598-023-31850-y
Circulating proteins to predict COVID-19 severity
Abstract
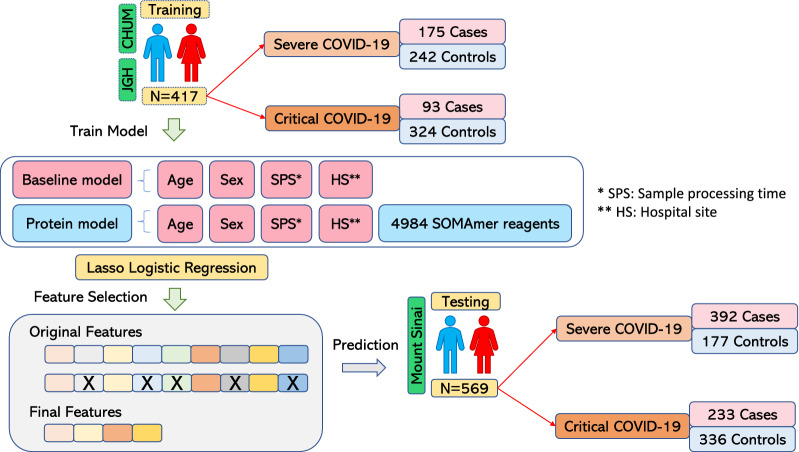
Predicting COVID-19 severity is difficult, and the biological pathways involved are not fully understood. To approach this problem, we measured 4701 circulating human protein abundances in two independent cohorts totaling 986 individuals. We then trained prediction models including protein abundances and clinical risk factors to predict COVID-19 severity in 417 subjects and tested these models in a separate cohort of 569 individuals. For severe COVID-19, a baseline model including age and sex provided an area under the receiver operator curve (AUC) of 65% in the test cohort. Selecting 92 proteins from the 4701 unique protein abundances improved the AUC to 88% in the training cohort, which remained relatively stable in the testing cohort at 86%, suggesting good generalizability. Proteins selected from different COVID-19 severity were enriched for cytokine and cytokine receptors, but more than half of the enriched pathways were not immune-related. Taken together, these findings suggest that circulating proteins measured at early stages of disease progression are reasonably accurate predictors of COVID-19 severity. Further research is needed to understand how to incorporate protein measurement into clinical care.
© 2023. The Author(s).
Conflict of interest statement
J.B.R. has served as an advisor to GlaxoSmithKline and Deerfield Capital and is the Founder of 5 Prime Sciences. The Lady Davis Institute has previously received funding from GlaxoSmithKline, Eli Lilly, and Biogen for research programs at Dr. Richards’ laboratory unrelated to this manuscript. C.P. and M.H. are employees of SomaLogic. All other authors do not have any conflict of interest. TN has received speaking fees from Boehringer Ingelheim for talks unrelated to this research. S.G. reports other research funding from Bristol-Myers Squibb, Boehringer-Ingelheim, Celgene, Genentech, Regeneron, and Takeda. S.G. reports other research funding from Bristol-Myers Squibb, Boehringer-Ingelheim, Celgene, Genentech, Regeneron, and Takeda.
Figures


References
-
- The COVID-19 Host Genetics Initiative. Mapping the human genetic architecture of COVID-19 by worldwide meta-analysis. medRxiv (2021) doi:10.1101/2021.03.10.21252820.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
