

Outcomes of Intramuscular Gluteal Augmentation With Implants Using Tumescent Local Anesthesia
- PMID: 37069350
- PMCID: PMC10582138
- DOI: 10.1007/s00266-023-03342-x
Outcomes of Intramuscular Gluteal Augmentation With Implants Using Tumescent Local Anesthesia
Abstract
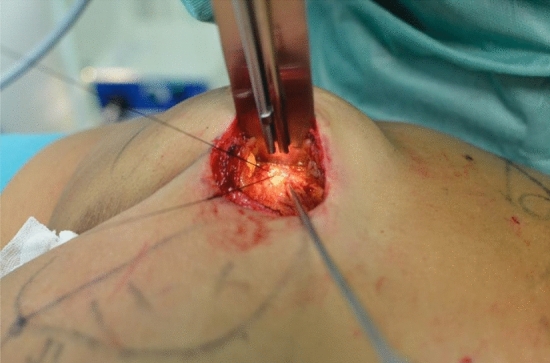
Background: Tumescent local anesthesia (TLA) describes the practice of injecting a very dilute solution of local anesthetic combined with epinephrine and sodium bicarbonate into the tissue until it becomes firm and tense to obtain local anesthesia and vasoconstriction. The use of TLA in augmentation intramuscular gluteoplasty has never been described for implants positioning. Advantages of the TLA technique include a reduction in blood loss through epinephrine-induced vasoconstriction and hydrostatic compression from the tumescent effect. We describe TLA technique for primary intramuscular gluteal augmentation, reporting our experience during the last 5 years.
Methods: From 2017 to 2021, 20 patients underwent bilateral primary gluteal augmentation under TLA and conscious sedation. The tumescent solution was prepared with 25 mL of 2% lidocaine, 8 mEq of sodium bicarbonate, and 1 mL of epinephrine (1 mg/1 mL) in 1000 mL of 0.9% saline solution. The solution was infiltrated with a cannula inside the gluteus maximus muscle intra-operatively.
Results: The mean age of the patients was 39, 15 years. The average amount of tumescent solution infiltrated was 240 mL per gluteus. Operating time was 1 h and 40 min, and recovery room time averaged 240 min. Major surgery-related complications were found in 15% of patients (2 hematomas and 1 seroma) and minor complications were described in a total of 8 patients (4 wound dehiscence and 1 dystrophic scar formation). No signs of adrenaline nor lidocaine toxicity were reported and conversion to general anesthesia was never required.
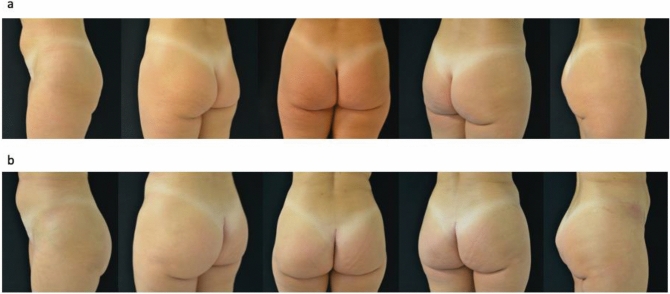
Conclusions: The tumescent local anesthesia technique represents a safe and efficacious technique for performing gluteal augmentation surgery with an intramuscular implant positioning. The advantages of this technique are safety, reasonable pain control during and after surgery and a low incidence of postoperative side effects due to general anesthesia avoidance.
Level of evidence iv: This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266 .
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures




References
-
- Robles JM, Tagliapietra JL, Grandi MA. Gluteoplastia de aumento: implante submuscular. Cir Plast Iberolatinoam. 1984;10(4):365–375.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
