

Incident type 2 diabetes attributable to suboptimal diet in 184 countries
- PMID: 37069363
- PMCID: PMC10115653
- DOI: 10.1038/s41591-023-02278-8
Incident type 2 diabetes attributable to suboptimal diet in 184 countries
Abstract
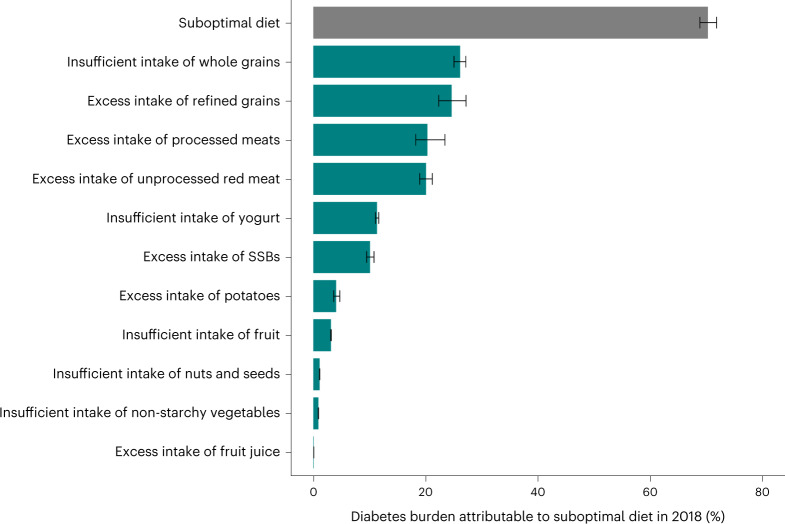
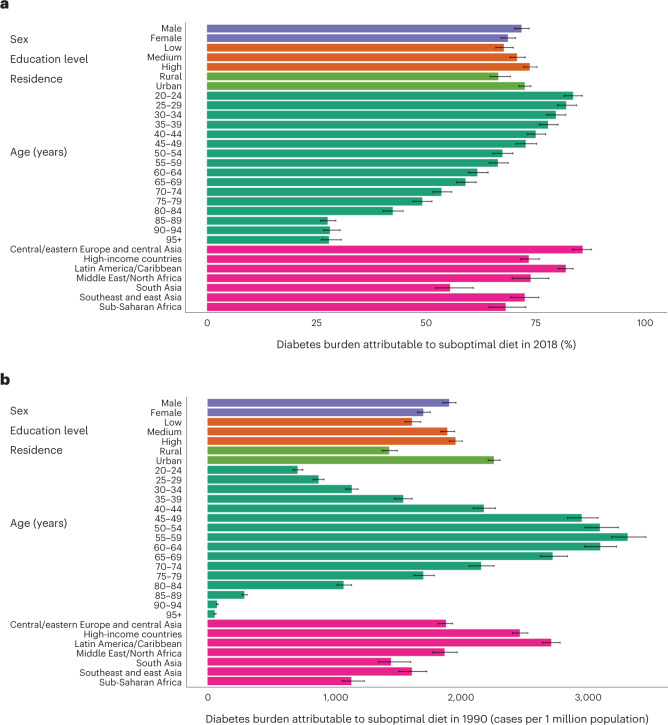
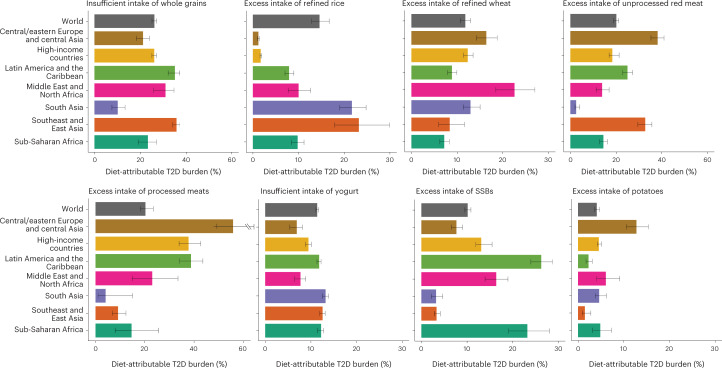
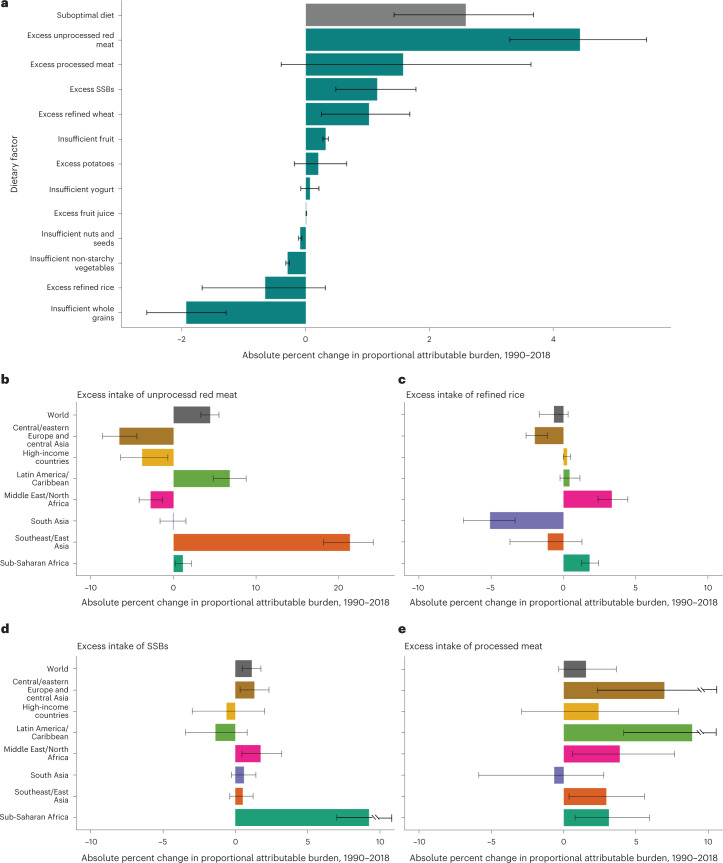
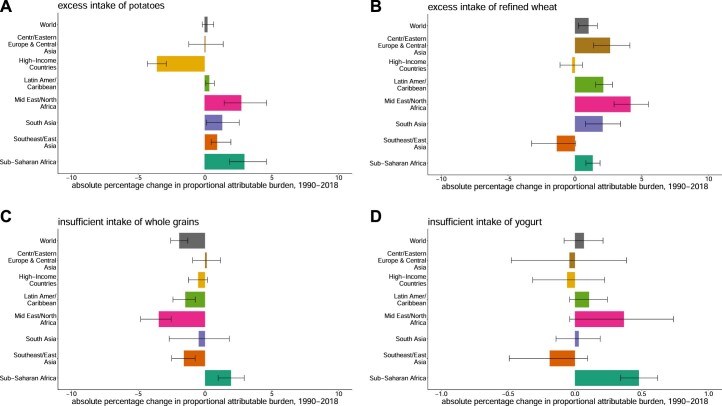
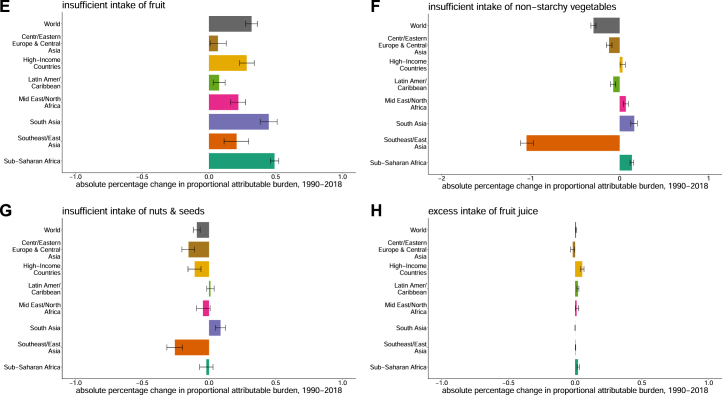
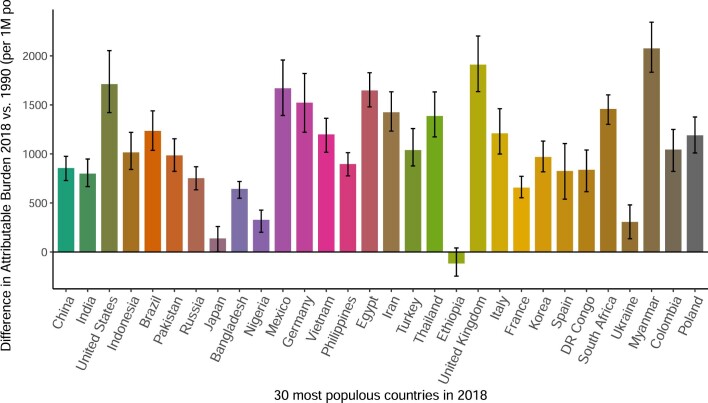
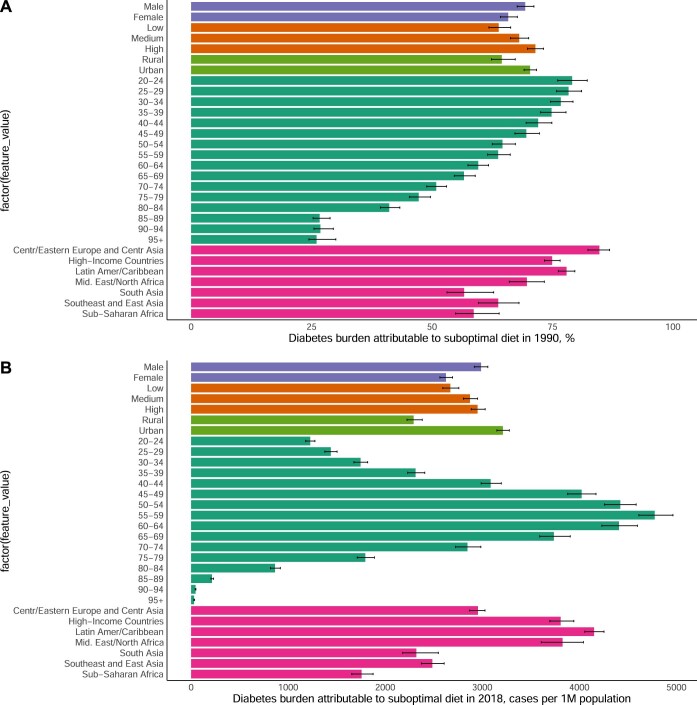
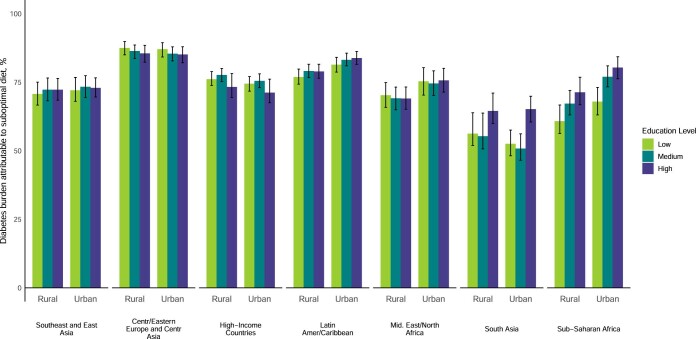
The global burden of diet-attributable type 2 diabetes (T2D) is not well established. This risk assessment model estimated T2D incidence among adults attributable to direct and body weight-mediated effects of 11 dietary factors in 184 countries in 1990 and 2018. In 2018, suboptimal intake of these dietary factors was estimated to be attributable to 14.1 million (95% uncertainty interval (UI), 13.8-14.4 million) incident T2D cases, representing 70.3% (68.8-71.8%) of new cases globally. Largest T2D burdens were attributable to insufficient whole-grain intake (26.1% (25.0-27.1%)), excess refined rice and wheat intake (24.6% (22.3-27.2%)) and excess processed meat intake (20.3% (18.3-23.5%)). Across regions, highest proportional burdens were in central and eastern Europe and central Asia (85.6% (83.4-87.7%)) and Latin America and the Caribbean (81.8% (80.1-83.4%)); and lowest proportional burdens were in South Asia (55.4% (52.1-60.7%)). Proportions of diet-attributable T2D were generally larger in men than in women and were inversely correlated with age. Diet-attributable T2D was generally larger among urban versus rural residents and higher versus lower educated individuals, except in high-income countries, central and eastern Europe and central Asia, where burdens were larger in rural residents and in lower educated individuals. Compared with 1990, global diet-attributable T2D increased by 2.6 absolute percentage points (8.6 million more cases) in 2018, with variation in these trends by world region and dietary factor. These findings inform nutritional priorities and clinical and public health planning to improve dietary quality and reduce T2D globally.
© 2023. The Author(s).
Conflict of interest statement
M. OHearn reports research funding from the Gates Foundation, as well as the National Institutes of Health and Vail Innovative Global Research and employment with Food Systems for the Future, outside of the submitted work. L. Lara-Castor reports research funding from the Gate Foundation, as well as the Consejo Nacional de Ciencia y Tecnologia (CONACyT), Friedman School of Nutrition Science and Policy and the American Heart Association, outside of the submitted work. V. Miller reports research funding from the Canadian Institutes of Health Research and the American Heart Association, outside of the submitted work. F. Cudhea, J. Zhang, and P. Shi report research funding form the Gates Foundation, as well as the National Institutes of Health, outside of the submitted work. J. Reedy reports research funding from the Gates Foundation, as well as the National Institutes of Health, Nestlé, Rockefeller Foundation, and Kaiser Permanent Fund at East Bay Community Foundation, outside of the submitted work. J. Wong reports research funding from the National Institutes of Health and membership in the US Preventative Services Task Force (unpaid) and the National Academies of Sciences, Engineering and Medicine Committee on Evaluating the Process to Develop the Dietary Guidelines for Americans, 2020–2025 (unpaid), outside the submitted work. C. Economos reports research funding from the United States Department of Agriculture, the National Institutes of Health, the JPB Foundation and Newman’s Own Foundation. She also reports her position as vice chair to the National Academies of Science Roundtable on Obesity Solutions (unpaid) and her prior advisory board position at Care/Of Scientific. None of the above relate to this paper. R. Micha reports research funding from the Gates Foundation, as well as the National Institutes of Health, Nestlé and Danone, outside the submitted work. She also reports consulting fees as IEG chair of the Global Nutrition Report, outside the submitted work. D. Mozaffarian reports funding from the National Institutes of Health, the Gates Foundation, the Rockefeller Foundation, Vail Innovative Global Research and the Kaiser Permanente Fund at East Bay Community Foundation; personal fees from Acasti Pharma, Barilla, Danone and Motif FoodWorks; is on the scientific advisory board for Beren Therapeutics, Brightseed, Calibrate, DiscernDx, Elysium Health, Filtricine, HumanCo, January, Perfect Day, Tiny Organics and (ended) Day Two and Season Health; has stock ownership in Calibrate and HumanCo; and receives chapter royalties from UpToDate.
Figures


Comment in
-
Government inaction and the preventable diabetes pandemic.Nat Med. 2023 Apr;29(4):791-792. doi: 10.1038/s41591-023-02259-x. Nat Med. 2023. PMID: 37069362 No abstract available.
References
-
- International Diabetes Federation. (2021). IDF Diabetes Atlas, 10th Edition Brussels, Belgium: International DiabetesFederation. http://www.diabetesatlas.org
-
- World Obesity Federation. World Obesity Atlas 2022https://www.worldobesity.org/resources/resource-library/world-obesity-at... (2022).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
