

In-hospital major adverse cardiovascular events after primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction: a retrospective study under the China chest pain center (standard center) treatment system
- PMID: 37069503
- PMCID: PMC10111847
- DOI: 10.1186/s12872-023-03214-x
In-hospital major adverse cardiovascular events after primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction: a retrospective study under the China chest pain center (standard center) treatment system
Abstract
Background: Patients with acute ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) are at high risk of major adverse cardiovascular events (MACE) despite timely treatment. This study aimed to investigate the independent predictors and their predictive value of in-hospital MACE after primary PCI in patients with acute STEMI under the China chest pain center (standard center) treatment system.
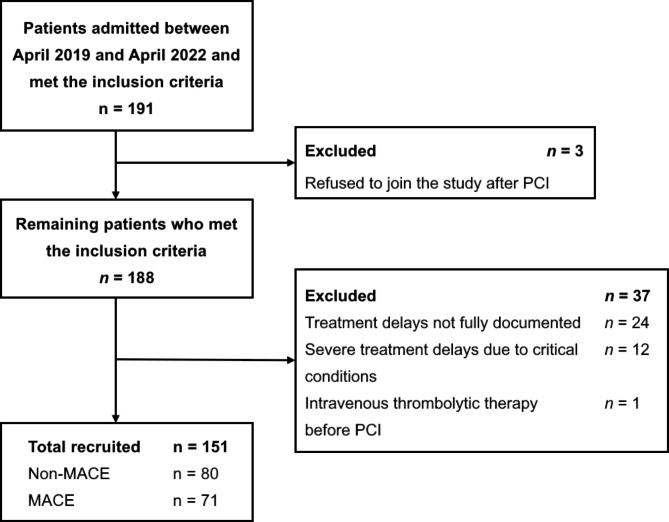
Methods: We performed a single-center, retrospective study of 151 patients with acute STEMI undergoing primary PCI. All patients were treated under the China chest pain center (standard center) treatment system. The data collected included general data, vital signs, auxiliary examination results, data related to interventional therapy, and various treatment delays. The primary endpoint was the in-hospital MACE defined as the composite of all-cause death, stroke, nonfatal recurrent myocardial infarction, new-onset heart failure, and malignant arrhythmias.
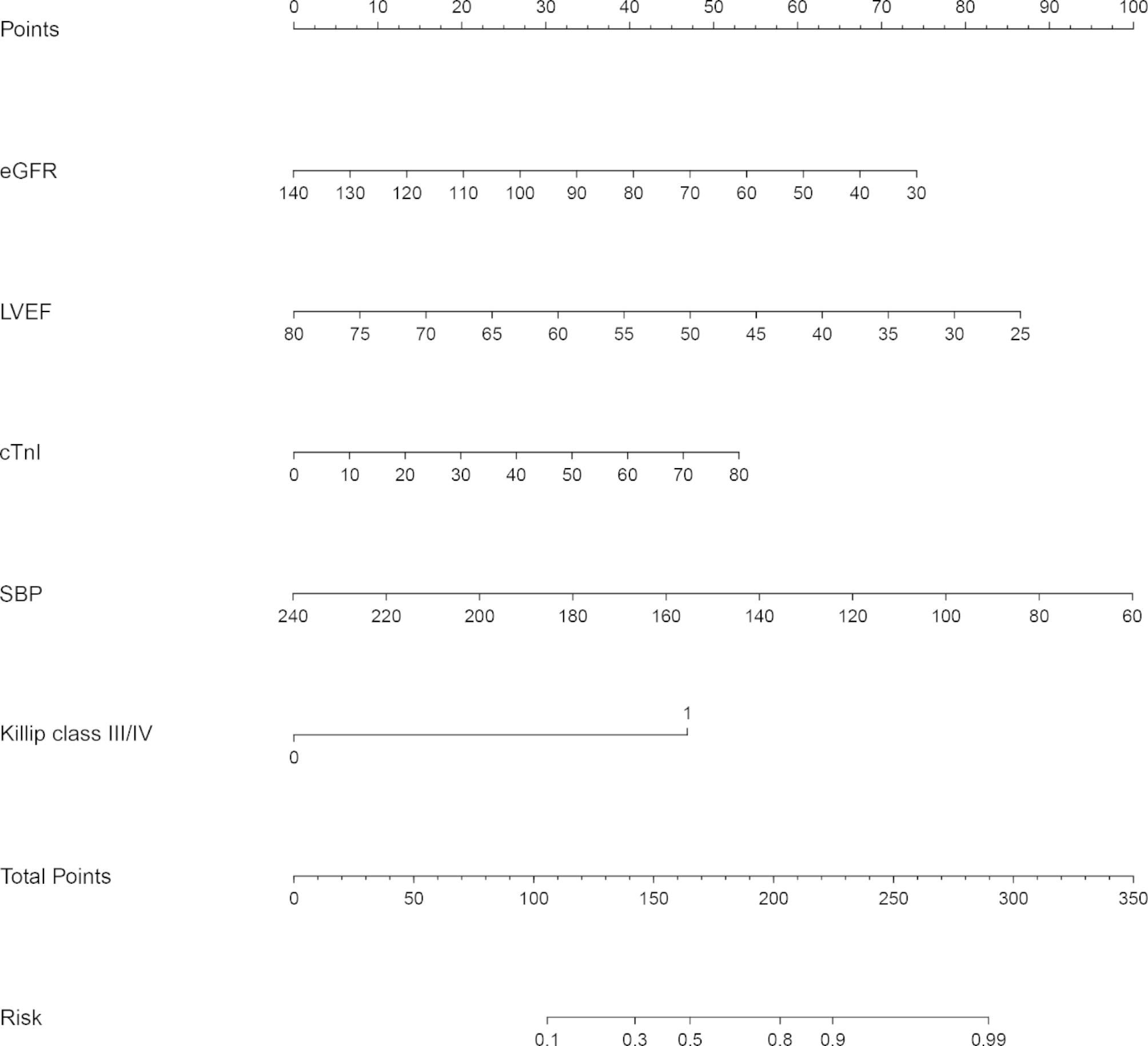
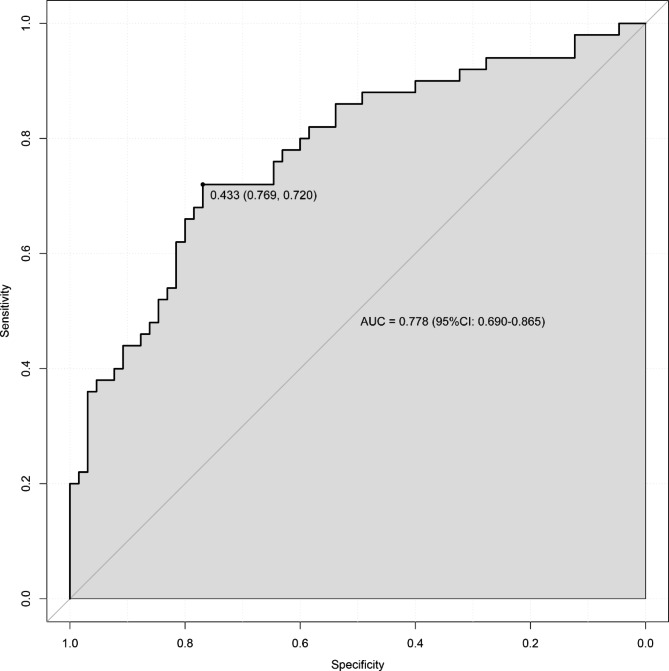
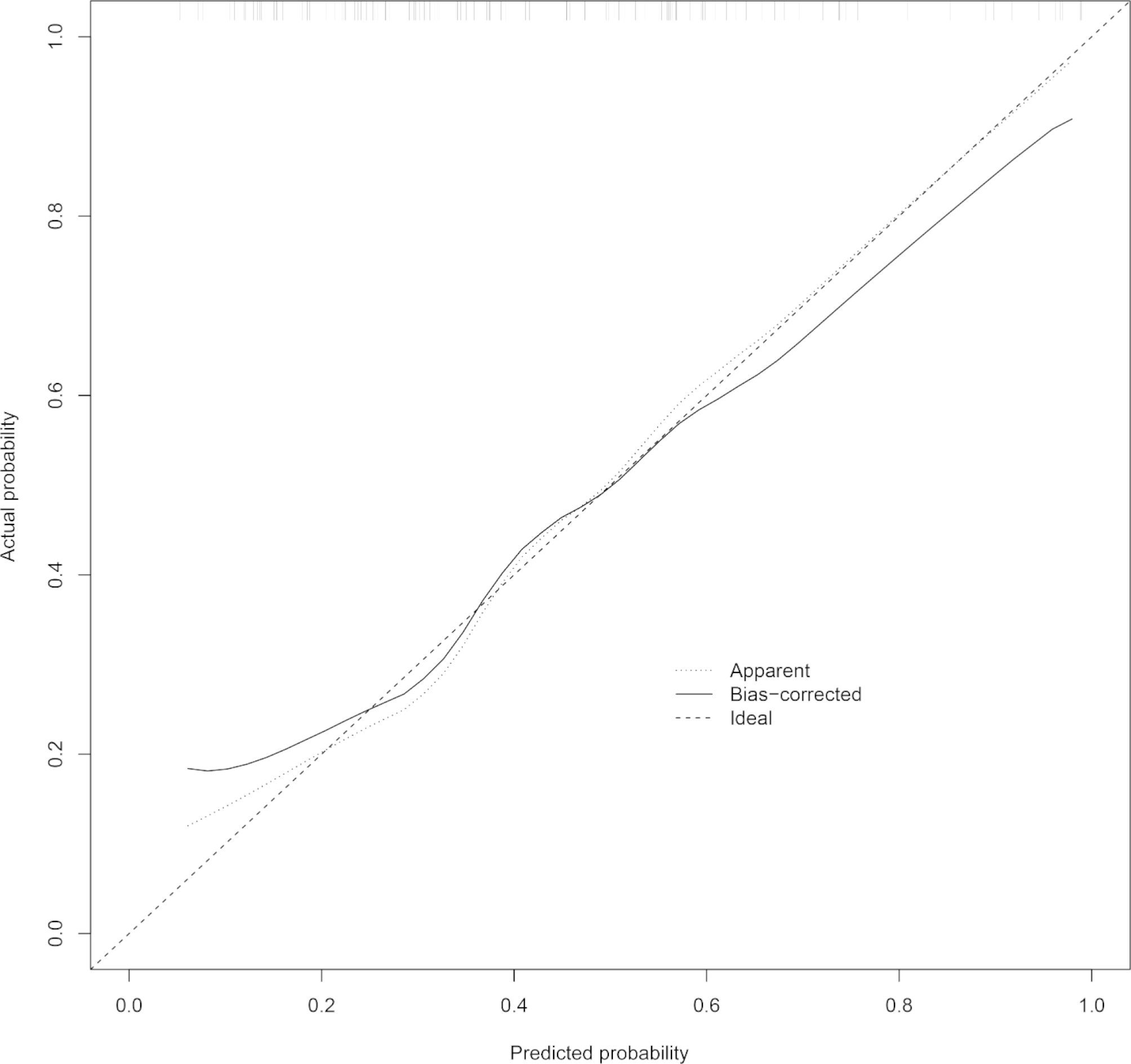
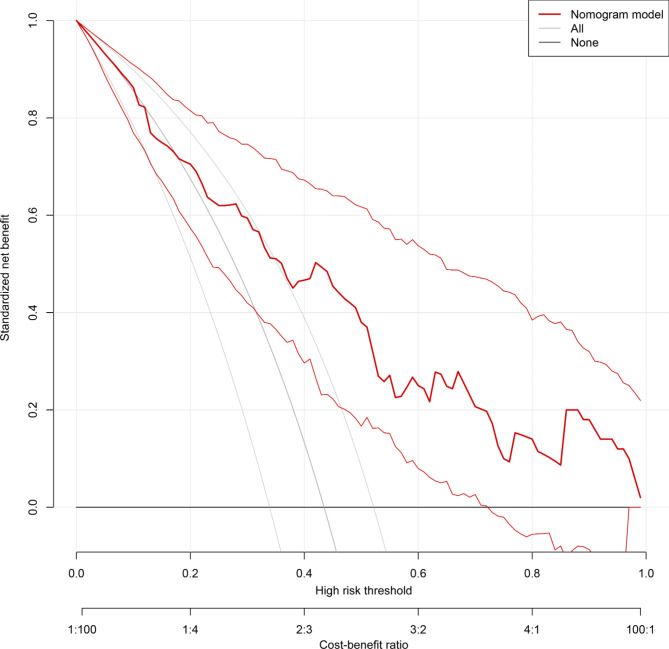
Results: In-hospital MACE occurred in 71 of 151 patients with acute STEMI undergoing primary PCI. Logistic regression analysis showed that age, cardiac troponin I (cTnI), serum creatinine (sCr), multivessel coronary artery disease, and Killip class III/IV were risk factors for in-hospital MACE, whereas estimated glomerular filtration rate (eGFR), left ventricular ejection fraction (LVEF), systolic blood pressure (SBP), diastolic blood pressure (DBP), were protective factors, with eGFR, LVEF, cTnI, SBP, and Killip class III/IV being independent predictors of in-hospital MACE. The prediction model had good discrimination with an area under the curve = 0. 778 (95%CI: 0.690-0.865). Good calibration and clinical utility were observed through the calibration and decision curves, respectively.
Conclusions: Our data suggest that eGFR, LVEF, cTnI, SBP, and Killip class III/IV independently predict in-hospital MACE after primary PCI in patients with acute STEMI, and the prediction model constructed based on the above factors could be useful for individual risk assessment and early management guidance.
Keywords: Chest pain center; Major adverse cardiovascular events; Percutaneous coronary intervention; ST-segment elevation myocardial infarction.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P, Lemesle G, Motreff P, Popovic B, Khalife K, et al. Acute myocardial infarction: changes in patient characteristics, management, and 6-Month Outcomes over a period of 20 years in the FAST-MI program (French Registry of Acute ST-Elevation or Non-ST-Elevation myocardial infarction) 1995 to 2015. Circulation. 2017;136(20):1908–19. doi: 10.1161/CIRCULATIONAHA.117.030798. - DOI - PubMed
-
- Jang SJ, Yeo I, Feldman DN, Cheung JW, Minutello RM, Singh HS, Bergman G, Wong SC, Kim LK. Associations between Hospital length of Stay, 30-Day readmission, and costs in ST-Segment-Elevation myocardial infarction after primary percutaneous coronary intervention: a Nationwide Readmissions Database Analysis. J Am Heart Assoc. 2020;9(11):e015503. doi: 10.1161/JAHA.119.015503. - DOI - PMC - PubMed
-
- Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, Li X, Wang L, Wang L, Liu Y, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the global burden of Disease Study 2017. Lancet. 2019;394(10204):1145–58. doi: 10.1016/S0140-6736(19)30427-1. - DOI - PMC - PubMed
-
- Li J, Li X, Wang Q, Hu S, Wang Y, Masoudi FA, Spertus JA, Krumholz HM, Jiang L. ST-segment elevation myocardial infarction in China from 2001 to 2011 (the China PEACE-Retrospective Acute Myocardial Infarction Study): a retrospective analysis of hospital data. Lancet. 2015;385(9966):441–51. doi: 10.1016/S0140-6736(14)60921-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
