

Spontaneous hemoperitoneum in the second and third trimester of pregnancy: two uncommon case reports at Tu Du Hospital, in Vietnam and a literature review
- PMID: 37069520
- PMCID: PMC10108475
- DOI: 10.1186/s12245-023-00498-w
Spontaneous hemoperitoneum in the second and third trimester of pregnancy: two uncommon case reports at Tu Du Hospital, in Vietnam and a literature review
Erratum in
-
Correction: Spontaneous hemoperitoneum in the second and third trimester of pregnancy: two uncommon case reports at Tu Du Hospital, in Vietnam and a literature review.Int J Emerg Med. 2023 Sep 5;16(1):55. doi: 10.1186/s12245-023-00535-8. Int J Emerg Med. 2023. PMID: 37670272 Free PMC article. No abstract available.
Abstract
Background: Spontaneous hemoperitoneum in pregnancy (SHiP) refers to fluid collection in the abdominal cavity with a vague presentation of clinical symptoms. Particularly, SHiP causes a life-threatening condition with the coexistence of intrauterine pregnancy, since this dangerous complication significantly increases the maternal and fetal mortality. Herein, we present two cases of nontraumatic SHiP in the second and third trimester of pregnancy, respectively.
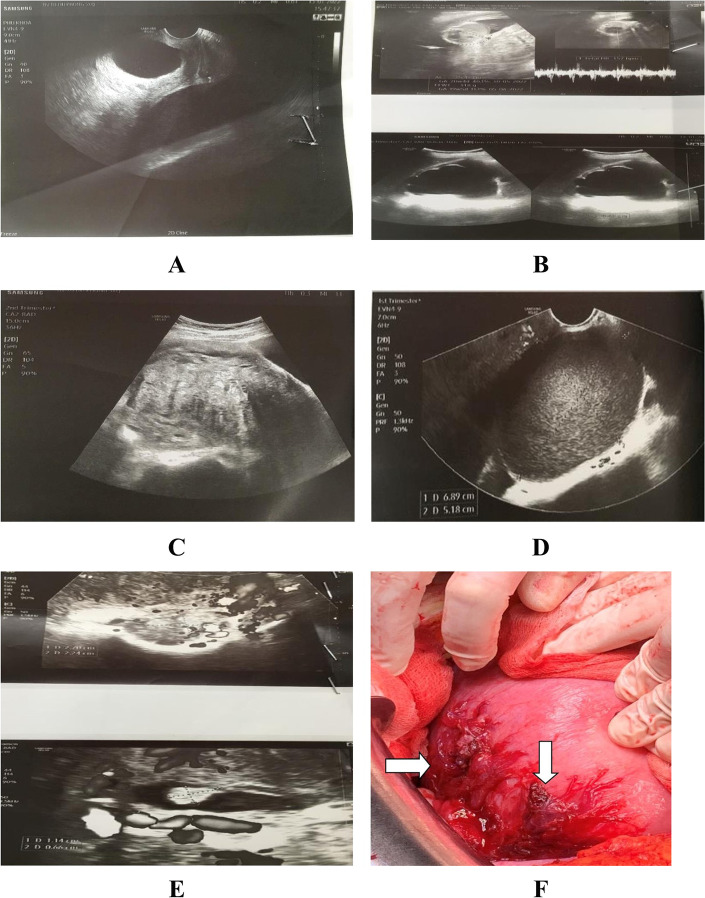
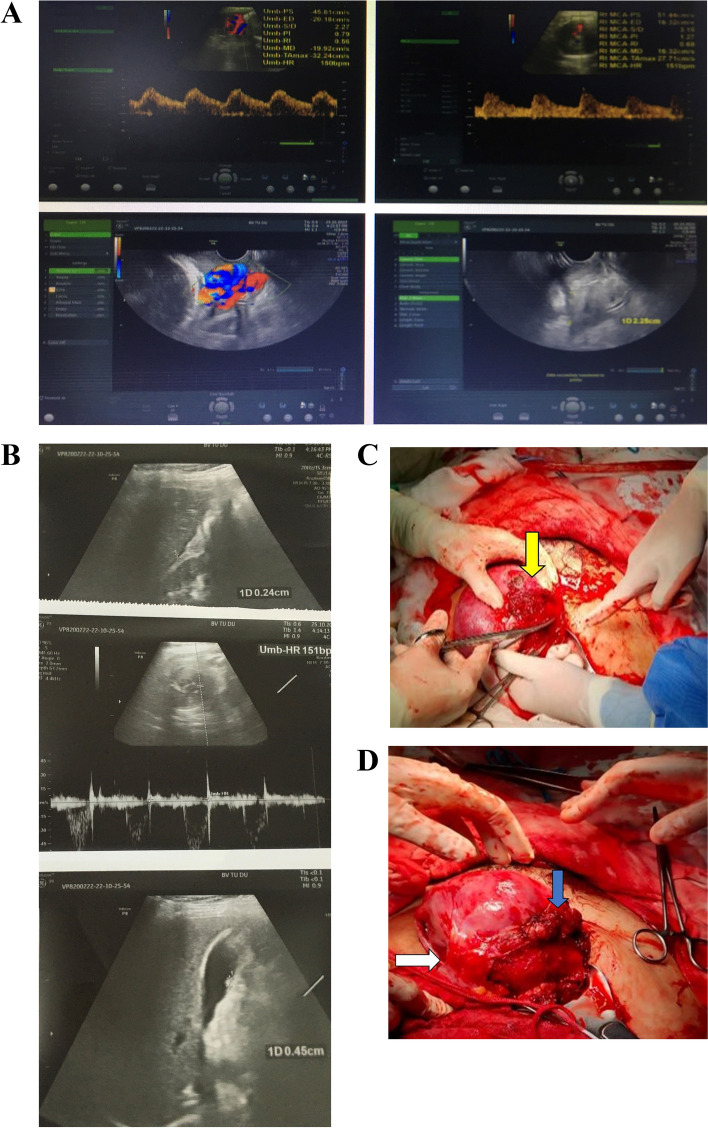
Case presentation: The pregnant woman in case 1 was admitted to our hospital owing to severe paroxysmal shoulder pain along with abdominal pain. Her medical history was remarkably recorded with endometriosis and adenomyosis. At the emergency room, an ultrasound scan revealed a live fetus corresponding to 21 weeks and 3 days and free fluid in the abdominal cavity. She was subsequently diagnosed with SHiP and underwent immediate laparotomy for hemostatic procedures. During the postpartum course, the patient was uneventfully monitored. Unfortunately, the patient delivered on the 4th postoperative day in spite of the initial administration of tocolytic agents and close monitoring. The primigravid woman in case 2 complained of lower abdominal pain and vaginal bleeding. The patient's history was noted with ovarian tumor removal. At admission, the sonography scan revealed free fluid in the abdominal cavity, a fetus at 34 weeks and 3 days gestational age with bradycardia of 70 bpm, and a laboratory test showed a low hemoglobin level. Thus, exploratory laparotomy and hysterotomy were performed at the same time due to fetal distress. The postpartum course was uneventful. The patient was discharged 5 days later.
Conclusions: In pregnant women with a history of endometriosis, adenomyosis, or ovarian tumor removal, acute abdominal pain combined with the presence of free fluid collection in the intraperitoneal cavity, and a decreased hemoglobin levels should be first assessed as SHiP originating from the spontaneous rupture of abnormal vascular proliferation. Proper management is strongly indicated for an emergent laparotomy to control the active bleeding point, thus increasing the survival rate for both mother and neonate.
Keywords: Emergency; Fetal death; Hemoglobin; Maternal mortality; Pregnancy; Spontaneous hemoperitoneum; Ultrasound.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests. This manuscript has not been published and is not under consideration for publication elsewhere. Additionally, all of the authors have approved the contents of this paper and have agreed to the journal’s submission policies.
Figures
Similar articles
-
A 41-Year-Old Woman with Spontaneous Hemoperitoneum in Pregnancy at 28 Weeks.Am J Case Rep. 2023 Jul 25;24:e939330. doi: 10.12659/AJCR.939330. Am J Case Rep. 2023. PMID: 37488914 Free PMC article.
-
Laparoscopic Management of Abdominal Pregnancy.J Minim Invasive Gynecol. 2017 Jul-Aug;24(5):724-725. doi: 10.1016/j.jmig.2017.01.023. Epub 2017 Feb 4. J Minim Invasive Gynecol. 2017. PMID: 28179200
-
Spontaneous hemoperitoneum in a 29-week pregnancy with a history of endometriosis: A case report and review of the literature.Int J Gynaecol Obstet. 2025 Apr;169(1):31-37. doi: 10.1002/ijgo.16006. Epub 2024 Nov 11. Int J Gynaecol Obstet. 2025. PMID: 39526833 Free PMC article. Review.
-
Guidelines for the Management of a Pregnant Trauma Patient.J Obstet Gynaecol Can. 2015 Jun;37(6):553-74. doi: 10.1016/s1701-2163(15)30232-2. J Obstet Gynaecol Can. 2015. PMID: 26334607 English, French.
-
Spontaneous hemoperitoneum in pregnancy: A life-threatening maternal and fetal complication of endometriosis.J Gynecol Obstet Hum Reprod. 2022 Sep;51(7):102415. doi: 10.1016/j.jogoh.2022.102415. Epub 2022 Jun 3. J Gynecol Obstet Hum Reprod. 2022. PMID: 35667589 Review.
Cited by
-
Spontaneous hemoperitoneum in the second trimester of pregnancy with a favorable outcome: a case report.J Int Med Res. 2025 Feb;53(2):3000605251317995. doi: 10.1177/03000605251317995. J Int Med Res. 2025. PMID: 40019121 Free PMC article.
-
A 41-Year-Old Woman with Spontaneous Hemoperitoneum in Pregnancy at 28 Weeks.Am J Case Rep. 2023 Jul 25;24:e939330. doi: 10.12659/AJCR.939330. Am J Case Rep. 2023. PMID: 37488914 Free PMC article.
-
Spontaneous Hemoperitoneum in Pregnancy: Masquerading as Acute Appendicitis.Cureus. 2023 Oct 14;15(10):e47040. doi: 10.7759/cureus.47040. eCollection 2023 Oct. Cureus. 2023. PMID: 38021831 Free PMC article.
-
Spontaneous haemoperitoneum in the second trimester of pregnancy.BMJ Case Rep. 2024 Jan 31;17(1):e258052. doi: 10.1136/bcr-2023-258052. BMJ Case Rep. 2024. PMID: 38296502
-
Correction: Spontaneous hemoperitoneum in the second and third trimester of pregnancy: two uncommon case reports at Tu Du Hospital, in Vietnam and a literature review.Int J Emerg Med. 2023 Sep 5;16(1):55. doi: 10.1186/s12245-023-00535-8. Int J Emerg Med. 2023. PMID: 37670272 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
