

Cost-effectiveness of the screen-and-treat strategies using HPV test linked to thermal ablation for cervical cancer prevention in China: a modeling study
- PMID: 37069602
- PMCID: PMC10111823
- DOI: 10.1186/s12916-023-02840-8
Cost-effectiveness of the screen-and-treat strategies using HPV test linked to thermal ablation for cervical cancer prevention in China: a modeling study
Abstract
Background: Self-sampling HPV test and thermal ablation are effective tools to increase screening coverage and treatment compliance for accelerating cervical cancer elimination. We assessed the cost-effectiveness of their combined strategies to inform accessible, affordable, and acceptable cervical cancer prevention strategies.
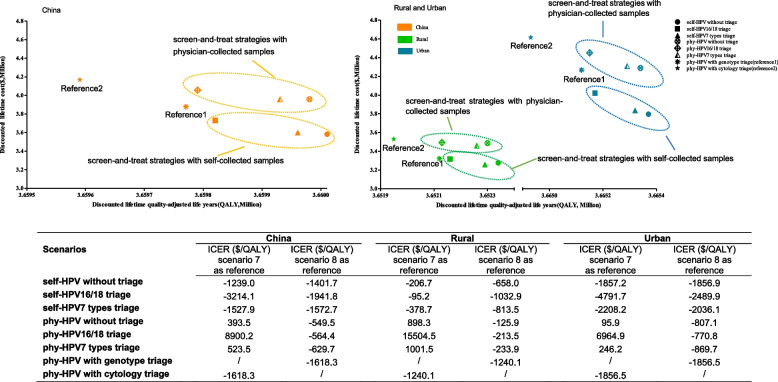
Methods: We developed a hybrid model to evaluate costs, health outcomes, and incremental cost-effectiveness ratios (ICER) of six screen-and-treat strategies combining HPV testing (self-sampling or physician-sampling), triage modalities (HPV genotyping, colposcopy or none) and thermal ablation, from a societal perspective. A designated initial cohort of 100,000 females born in 2015 was considered. Strategies with an ICER less than the Chinese gross domestic product (GDP) per capita ($10,350) were considered highly cost-effective.
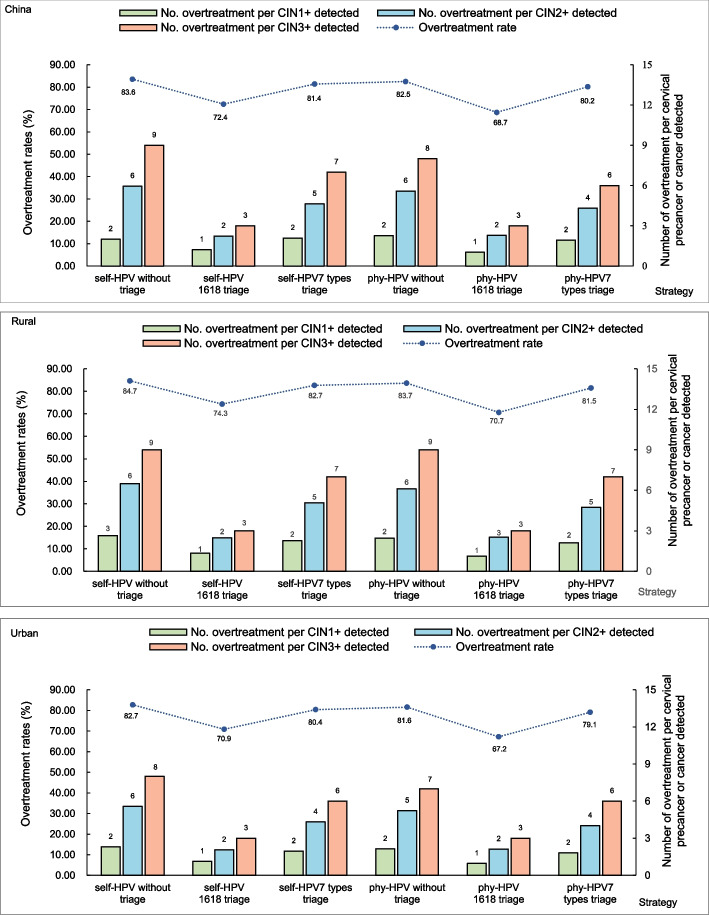
Results: Compared with current strategies in China (physician-HPV with genotype or cytology triage), all screen-and-treat strategies are cost-effective and self-HPV without triage is optimal with the most incremental quality-adjusted life-years (QALYs) gained (220 to 440) in rural and urban China. Each screen-and-treat strategy based on self-collected samples is cost-saving compared with current strategies (-$818,430 to -$3540) whereas more costs are incurred using physician-collected samples compared with current physician-HPV with genotype triage (+$20,840 to +$182,840). For screen-and-treat strategies without triage, more costs (+$9404 to +$380,217) would be invested in the screening and treatment of precancerous lesions rather than the cancer treatment compared with the current screening strategies. Notably, however, more than 81.6% of HPV-positive women would be overtreated. If triaged with HPV 7 types or HPV16/18 genotypes, 79.1% or 67.2% (respectively) of HPV-positive women would be overtreated with fewer cancer cases avoided (19 cases or 69 cases).
Conclusions: Screen-and-treat strategy using self-sampling HPV test linked to thermal ablation could be the most cost-effective for cervical cancer prevention in China. Additional triage with quality-assured performance could reduce overtreatment and remains highly cost-effective compared with current strategies.
Keywords: Cervical cancer; Cost-effectiveness; HPV test; Screen and treat; Thermal ablation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing financial interests.
Figures


References
-
- World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva, Switzerland. 2020. https://apps.who.int/iris/handle/10665/336583. Accessed 18 Oct 2022.
-
- Simms KT, Steinberg J, Caruana M, et al. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020–99: a modelling study. Lancet Oncol. 2019;20:394–407. doi: 10.1016/S1470-2045(18)30836-2. - DOI - PubMed
