

Evaluation of Latex Immunoturbidimetric Assay Thresholds and HIT in Cardiothoracic Surgery
- PMID: 37069794
- PMCID: PMC10123911
- DOI: 10.1177/10760296231166370
Evaluation of Latex Immunoturbidimetric Assay Thresholds and HIT in Cardiothoracic Surgery
Erratum in
-
Corrigendum to Evaluation of Latex Immunoturbidimetric Assay Thresholds and HIT in Cardiothoracic Surgery.Clin Appl Thromb Hemost. 2023 Jan-Dec;29:10760296231207240. doi: 10.1177/10760296231207240. Clin Appl Thromb Hemost. 2023. PMID: 37880958 Free PMC article. No abstract available.
Abstract
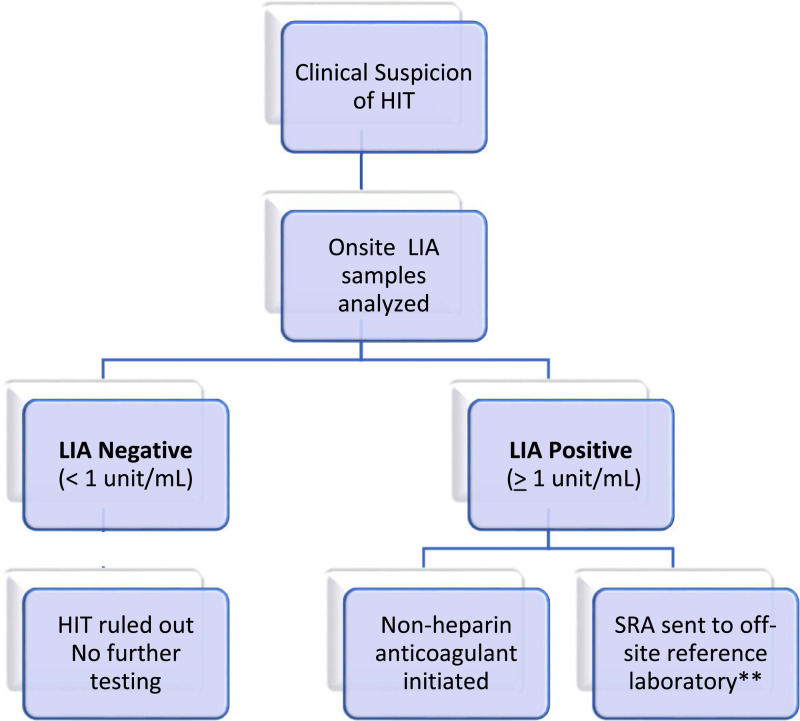
Background: Heparin-induced thrombocytopenia (HIT) is a common differential diagnosis in cardiothoracic surgery. The latex immunoturbidimetric assay (LIA) is an enhanced immunoassay that has recently been introduced for the detection of total HIT immunoglobulin and retains a higher specificity of 95% compared to the enzyme-linked immunosorbent assay.
Objectives: To investigate if a semiquantitative relationship exists between increasing LIA levels beyond the current positivity threshold and its correlation to positive serotonin release assay results in cardiothoracic surgery.
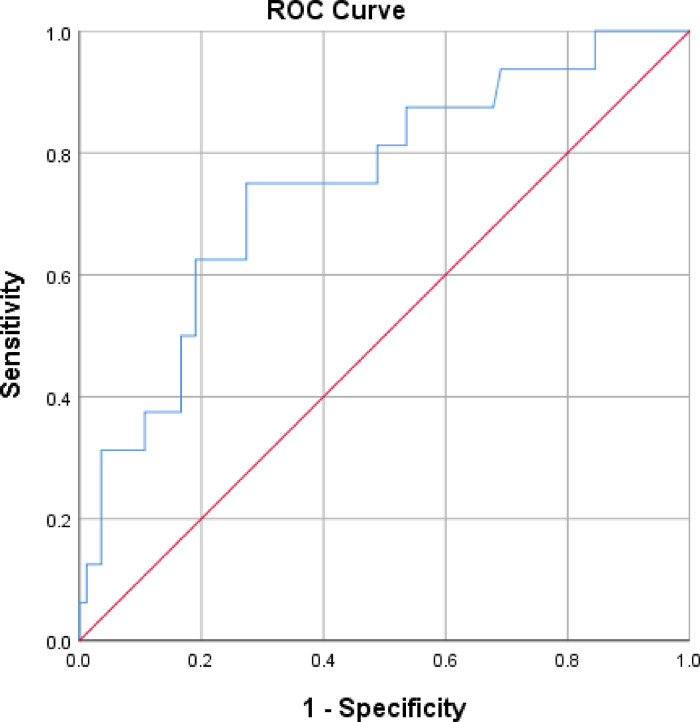
Methods: This was a multicenter, observational cohort of cardiothoracic surgery patients initiated on anticoagulation with heparin-based products. To conduct sensitivity and specificity analysis of LIA values, HIT positive was defined as a LIA value ≥1 unit/mL and HIT negative was defined as a LIA level <1 unit/mL. A receiver operating characteristic (ROC) analysis was utilized to evaluate the predictive performance of the LIA.
Results: At manufactures' cutoffs of ≥1.0 unit/mL, LIA sensitivity and specificity was 93.8% and 22%, respectively, yielding a false positive rate of 78%. At a higher cutoff of 4.5 units/mL, LIA sensitivity and specificity was 75% and 71%, respectively, yielding a false positive rate of 29% and an area under the ROC curve of 0.75 (P = .01; 95% confidence interval: 0.621-0.889). Bivalirudin was initiated in 84.6% of false positive LIA results.
Conclusion: This study suggests that the diagnostic accuracy of the LIA can be optimized by increasing the LIA positivity threshold. Proposing a higher LIA cutoff, may mitigate unwarranted anticoagulation and bleeding outcomes.
Keywords: bioassay; cardiac surgery; heparin-induced thrombocytopenia; immunology.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Warkentin TE, Sheppard JA, Horsewood P, et al. Impact of the patient population on the risk for heparin-induced thrombocytopenia. Blood. 2000;96(05):1703-1708. - PubMed
-
- Greinacher A, Selleng K. Thrombocytopenia in the intensive care unit patient. Hematol Am Soc Hematol Educ Program. 2010;2010(1):135-143. - PubMed
-
- Parker RI. Etiology and significance of thrombocytopenia in critically ill patients. Crit Care Clin. 2012;28(3):399-411. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
