

Giant Cellulitis-Like Sweet Syndrome Masquerading As Cellulitis and Shingles: A Case Report and Literature Review
- PMID: 37069879
- PMCID: PMC10105525
- DOI: 10.7759/cureus.36232
Giant Cellulitis-Like Sweet Syndrome Masquerading As Cellulitis and Shingles: A Case Report and Literature Review
Abstract
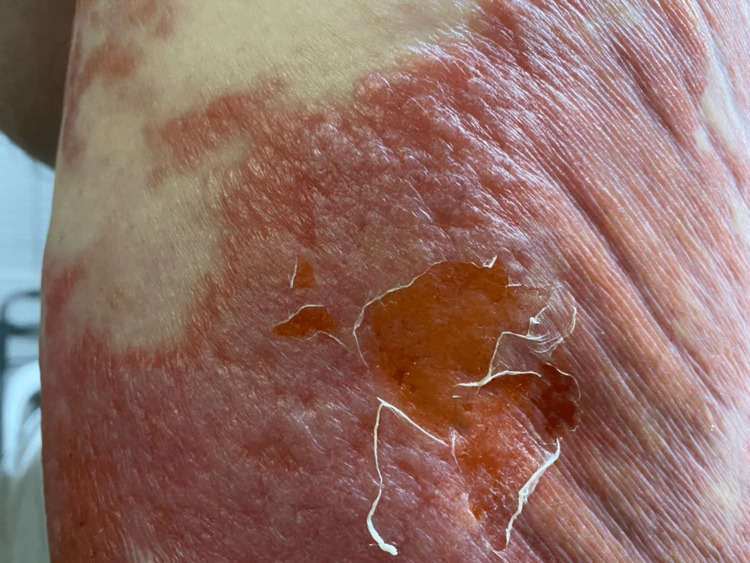
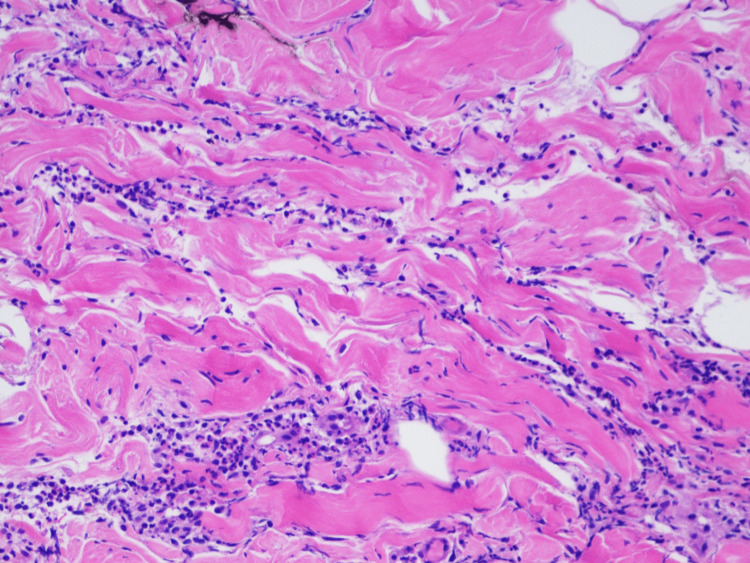
Sweet syndrome (SS) is also known as acute febrile neutrophilic dermatoses. Clinically, SS features fever, arthralgias, and the sudden onset of an erythematous rash. The morphologies of skin lesions in SS are heterogenous, varying from papules, plaques, and nodules to hemorrhagic bullae, which sometimes makes the diagnosis of SS more challenging. We report a 62-year-old obese male with a history of chronic myeloid leukemia in remission for 10 years who presented with a rash for five days. The patient reported prodromal flu-like symptoms with subjective fever, malaise, cough, and nasal congestion followed by a sudden onset, painful, non-pruritic rash. The rash was associated with bilateral hip arthralgias and abdominal pain. The patient denied any recent travel, exposure to sick contacts, or the use of any new medications. Physical examination showed a well-demarcated, non-blanching, confluent, erythematous plaque involving the bilateral buttocks and extending to the lower back and flanks with coalescent "juicy"-appearing plaques and flaccid bullae. No oral or mucosal involvement was noted. Laboratory investigations revealed mild leukocytosis, elevated inflammatory markers, and acute kidney injury. The patient was started on antibiotics given the cellulitis-like skin lesions, leukocytosis with neutrophilia, and elevated inflammatory markers. Dermatology was consulted, who attributed the patient's rash to shingles and recommended initiating acyclovir and obtaining a skin biopsy. However, the patient's rash and arthralgias worsened with anti-viral treatment while awaiting pathology results. Antinuclear antibodies, complement, human immunodeficiency virus, hepatitis panel, blood cultures, and tumor markers were all negative. Flow cytometry showed no evidence of hematopoietic neoplasms. The skin punch biopsy revealed dense neutrophilic infiltration in the dermis with no evidence of leukocytoclastic vasculitis, consistent with acute neutrophilic dermatoses. The diagnosis of giant cellulitis-like Sweet syndrome was established, and the patient was started on prednisone 60 milligrams daily. His symptoms improved promptly with steroid treatment. Our case suggests that SS can camouflage a wide spectrum of diseases, including cellulitis, shingles, vasculitis, drug eruptions, leukemia cutis, and sarcoidosis, which emphasizes the importance of keeping a high index of suspicion for SS when assessing the clinical constellations of fever, neutrophilia, and erythematous plaques suggesting atypical cellulitis. Approximately 21% of Sweet syndrome is associated with malignancy. Sweet syndrome can precede, concur with, or follow the onset of malignancy. Due to the lack of a systematic approach to patients with SS, under-investigation and diagnostic delays are common. Therefore, further screening and continuous monitoring in patients with SS becomes especially important in facilitating the early detection of a potential underlying malignancy and assists in initiating adequate therapy.
Keywords: acute febrile neutrophilic dermatosis; acute myeloid leukemia (aml); cellulitis; chronic myeloid leukemia; giant cellulitis like sweet syndrome; shingles; sweet syndrome.
Copyright © 2023, Li et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Giant cellulitis-like Sweet syndrome: An underrecognized clinical variant mimicking skin and soft tissue infection.IDCases. 2020 Jun 16;21:e00874. doi: 10.1016/j.idcr.2020.e00874. eCollection 2020. IDCases. 2020. PMID: 32596132 Free PMC article.
-
Giant cellulitis-like Sweet syndrome mimicking cellulitis: a case report.J Med Case Rep. 2024 Oct 11;18(1):492. doi: 10.1186/s13256-024-04848-x. J Med Case Rep. 2024. PMID: 39390463 Free PMC article.
-
Recurrent Idiopathic Sweet Syndrome - Case Report and Literature Review.Curr Health Sci J. 2020 Jan-Mar;46(1):90-98. doi: 10.12865/CHSJ.46.01.12. Epub 2020 Mar 31. Curr Health Sci J. 2020. PMID: 32637170 Free PMC article.
-
Recurrent Malignancy-Associated Atypical Neutrophilic Dermatosis With Noninfectious Shock.Am J Med Sci. 2017 Dec;354(6):626-632. doi: 10.1016/j.amjms.2016.10.003. Epub 2016 Oct 20. Am J Med Sci. 2017. PMID: 29208261 Review.
-
[Cutaneous Manifestations of Sweet Disease].Brain Nerve. 2019 Apr;71(4):334-338. doi: 10.11477/mf.1416201271. Brain Nerve. 2019. PMID: 30988216 Review. Japanese.
Cited by
-
Giant cellulitis-like Sweet syndrome with myofasciitis: Multimodality imaging findings and streptococcal trigger.Radiol Case Rep. 2025 Apr 5;20(6):3092-3098. doi: 10.1016/j.radcr.2025.03.039. eCollection 2025 Jun. Radiol Case Rep. 2025. PMID: 40242382 Free PMC article.
References
-
- An acute febrile neutrophilic dermatosis. Sweet RD. Br J Dermatol. 1964;76:349–356. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials