

Mohs Surgery for Periocular Basal Cell Carcinoma Without a Mohs Surgeon: The First Series in Hong Kong
- PMID: 37069888
- PMCID: PMC10105576
- DOI: 10.7759/cureus.36235
Mohs Surgery for Periocular Basal Cell Carcinoma Without a Mohs Surgeon: The First Series in Hong Kong
Abstract
Purpose To report the first series of Mohs micrographic surgery (MMS) in Hong Kong, where the roles of a Mohs surgeon were shared and coordinated by a "mobile" surgeon.
Methods design: Prospective non-comparative interventional case series.
Subjects: 20 consecutive Chinese patients (10 male, age 78.5+10.4 years, range 55-91 years) with primary periocular basal cell carcinoma (pBCC) referred to the university oculoplastic unit between October 2007 and August 2013.
Intervention: MMS were conducted according to a streamlined standard operating procedure emphasizing surgeon-driven mapping, specimen orientation, and on-site clinico-histological correlation with the dermatopathologist at the frozen-section laboratory.
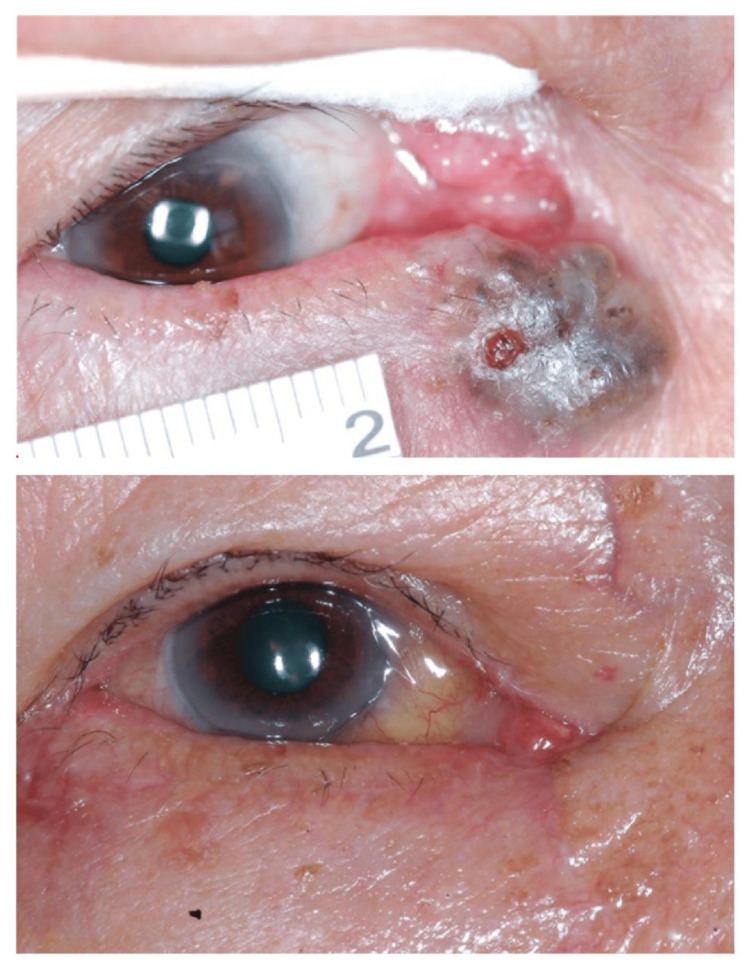
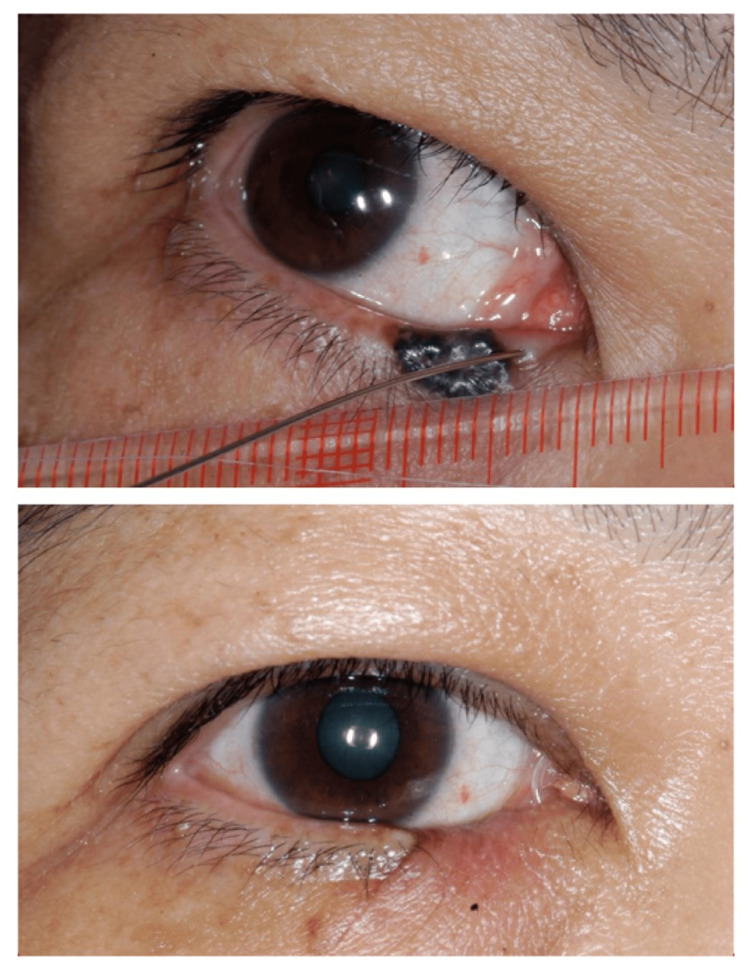
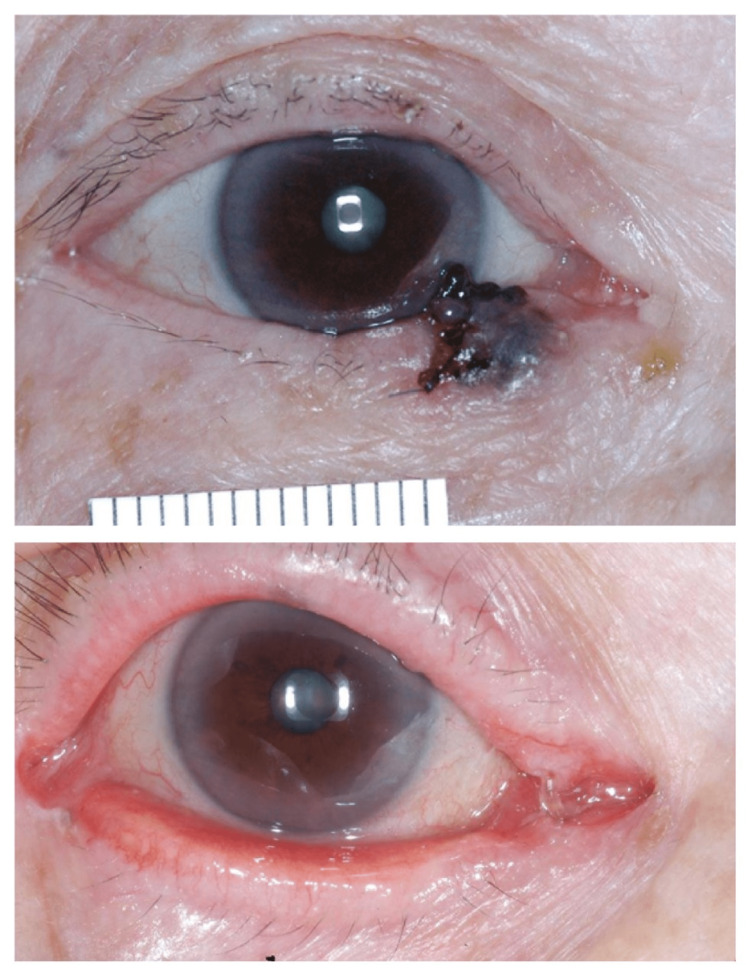
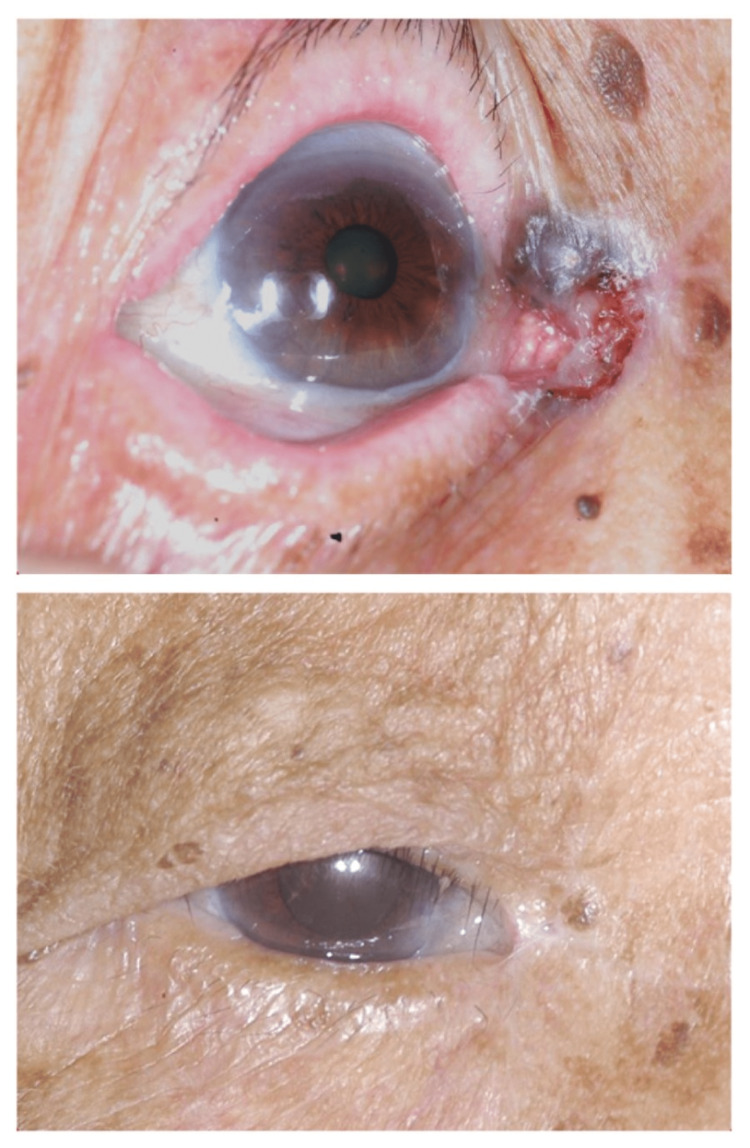
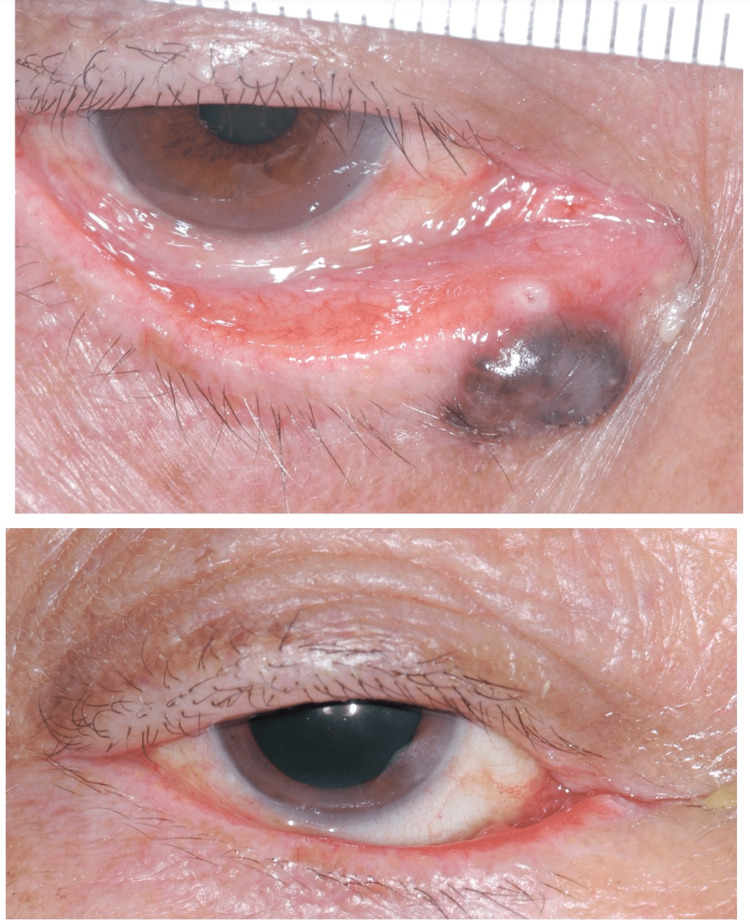
Main outcome measures: Clinical and histological characteristics of tumors, layers of Mohs procedures, complications, and biopsy-confirmed recurrence at the same location. Results All 20 patients received MMS as planned. Sixteen pBCCs (80%) were diffusely pigmented, and three (15%) were focally pigmented. Sixteen were also nodular. The average tumor diameter was 7+3 (3-15) mm. Seven (35%) were within 2 mm of the punctum. Histologically, 11 (55%) were nodules, and four (20%) were superficial. An average of 1.8+0.8 Mohs levels were performed. Apart from the initial two patients, who required four and three levels, respectively, seven (35%) patients were cleared after the first level of MMS using a 1mm clinical margin. The remaining 11 patients required two levels with an additional 1-2mm margin, but only focally as guided histologically. Defects in 16 patients (80%) were reconstructed by local flaps, two by direct closure, and two with pentagon closure. Among the seven patients with pericanalicular BCC, three patients had their remaining canaliculi successfully intubated, while two developed stenotic upper and two lower punctae postoperatively. One patient had prolonged wound healing. Three patients had lid margin notching, two had medial ectropion, one had medial canthal rounding, and two had lateral canthal dystopia. No recurrence was detected at a mean follow-up of 80+23 months (43 to 113 months) in all patients. Conclusions MMS was successfully introduced in Hong Kong without a Mohs surgeon. Providing complete microscopic margin control and preserving tissues, it was proven to be a valuable treatment option for pBCC. Our multidisciplinary protocol demonstrated that these merits are possible and warrant validation in other resource-limited healthcare settings.
Keywords: asians; basal cell carcinoma; eyelid; mohs surgery; periocular.
Copyright © 2023, Chan et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
The Australian Mohs database, part II: periocular basal cell carcinoma outcome at 5-year follow-up.Ophthalmology. 2004 Apr;111(4):631-6. doi: 10.1016/j.ophtha.2003.11.004. Ophthalmology. 2004. PMID: 15051193
-
Periocular Mohs micrographic surgery: Results of a dual-site day-surgery service.Orbit. 2001 Sep;20(3):209-215. doi: 10.1076/orbi.20.3.209.2627. Orbit. 2001. PMID: 12045913
-
Recurrence of periocular basal cell carcinoma and squamous cell carcinoma after Mohs micrographic surgery: a retrospective cohort study.Br J Dermatol. 2019 May;180(5):1176-1182. doi: 10.1111/bjd.17516. Epub 2019 Feb 10. Br J Dermatol. 2019. PMID: 30536656 Free PMC article.
-
Sebaceous carcinoma of the eyelids treated by mohs micrographic surgery: report of nine cases with review of the literature.Dermatol Surg. 2002 Jul;28(7):623-31. doi: 10.1046/j.1524-4725.2002.01306.x. Dermatol Surg. 2002. PMID: 12135523 Review.
-
The Use of Dermoscopy in the Delineation of Basal Cell Carcinoma for Mohs Micrographic Surgery: a Systematic Review With Meta-Analysis.Dermatol Pract Concept. 2022 Oct 1;12(4):e2022176. doi: 10.5826/dpc.1204a176. eCollection 2022 Nov. Dermatol Pract Concept. 2022. PMID: 36534540 Free PMC article. Review.
Cited by
-
A Systematic Review and Meta-Analysis of Ocular and Periocular Basal Cell Carcinoma with First-Time Description of Dermoscopic and Reflectance Confocal Microscopy Features of Caruncle Basal Cell Carcinoma.Diagnostics (Basel). 2025 May 14;15(10):1244. doi: 10.3390/diagnostics15101244. Diagnostics (Basel). 2025. PMID: 40428237 Free PMC article. Review.
-
Mohs micrographic surgery for basal cell carcinoma in Singapore: A retrospective review.JAAD Int. 2024 Aug 23;17:167-169. doi: 10.1016/j.jdin.2024.07.016. eCollection 2024 Dec. JAAD Int. 2024. PMID: 39525841 Free PMC article. No abstract available.
References
-
- Basal-cell carcinoma. Rubin AI, Chen EH, Ratner D. N Engl J Med. 2005;353:2262–2269. - PubMed
-
- A systematic review of worldwide incidence of nonmelanoma skin cancer. Lomas A, Leonardi-Bee J, Bath-Hextall F. Br J Dermatol. 2012;166:1069–1080. - PubMed
-
- Skin cancer in skin of color. Gloster HM Jr, Neal K. J Am Acad Dermatol. 2006;55:741–760. - PubMed
-
- Hospital Authority: Cancer statistics. 2018. http://www3.ha.org.hk/cancereg/statistics.html http://www3.ha.org.hk/cancereg/statistics.html
-
- Incidence of eyelid cancers in Taiwan: a 21-year review. Lin HY, Cheng CY, Hsu WM, Kao WH, Chou P. Ophthalmology. 2006;113:2101–2107. - PubMed
LinkOut - more resources
Full Text Sources