

Effects of Ertugliflozin on Kidney Outcomes in Patients With Heart Failure at Baseline in the Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes (VERTIS CV) Trial
- PMID: 37069970
- PMCID: PMC10105061
- DOI: 10.1016/j.ekir.2023.01.011
Effects of Ertugliflozin on Kidney Outcomes in Patients With Heart Failure at Baseline in the Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes (VERTIS CV) Trial
Abstract
Introduction: In the eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes (VERTIS CV) trial (NCT01986881), patients with type 2 diabetes mellitus (T2DM) and atherosclerotic cardiovascular disease (ASCVD) were randomized (1:1:1) to placebo, ertugliflozin 5 mg or 15 mg (doses pooled for analyses as prospectively planned). In this post hoc analysis, the effects of ertugliflozin on kidney outcomes were assessed in analyses stratified by baseline heart failure (HF).
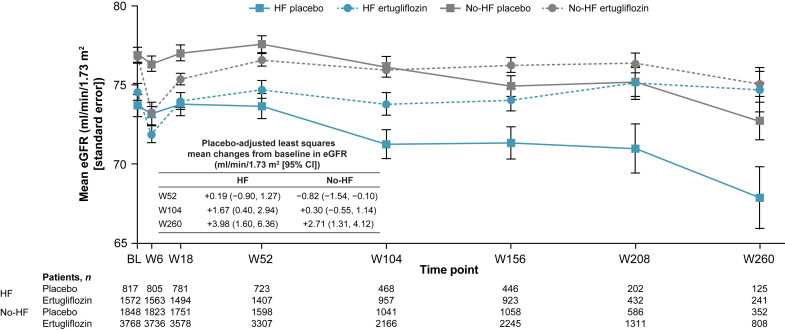
Methods: Baseline HF was defined as a history of HF or prerandomization left ventricular ejection fraction ≤45%. Outcomes included estimated glomerular filtration rate (eGFR) over time, total 5-year eGFR slopes and time to first event of a prespecified exploratory kidney composite outcome of sustained ≥40% decrease from baseline eGFR, chronic kidney replacement therapy, or kidney death. All analyses were stratified by baseline HF status.
Results: Compared with no-HF at baseline (n = 5807; 70.4%), patients with HF (n = 2439; 29.6%) had a notably faster rate of eGFR decline, which is unlikely to be explained by the slightly lower baseline eGFR in that group. Ertugliflozin treatment resulted in a slower rate of eGFR decline in both subgroups; total placebo-adjusted 5-year eGFR slopes (ml/min per 1.73 m2 per year [95% confidence intervals; CI]) were 0.96 (0.67-1.24) and 0.95 (0.76-1.14) for HF and no-HF subgroups, respectively. The placebo HF (vs. placebo no-HF) subgroup had a higher incidence of the composite kidney outcome (35/834 [4.20%] vs. 50/1913 [2.61%]). Hazard ratios (95% CI) for the effect of ertugliflozin on the composite kidney outcome did not differ significantly between HF and no-HF subgroups: 0.53 (0.33-0.84) and 0.76 (0.53-1.08), respectively (P interaction = 0.22).
Conclusion: Although patients with HF at baseline had a faster rate of eGFR decline in VERTIS CV, the beneficial effects of ertugliflozin on kidney outcomes did not differ when stratified by baseline HF.
Keywords: albuminuria; diabetic kidney disease; ertugliflozin; heart failure; sodium–glucose cotransporter 2 inhibitor; type 2 diabetes mellitus.
© 2023 [Author/Employing Institution].
Figures



Similar articles
-
Heart and Kidney Outcomes With Ertugliflozin in People with Non-albuminuric Diabetic Kidney Disease: A post hoc Analysis from the Randomized VERTIS CV Trial.Kidney Int Rep. 2022 May 13;7(8):1782-1792. doi: 10.1016/j.ekir.2022.05.007. eCollection 2022 Aug. Kidney Int Rep. 2022. PMID: 35967112 Free PMC article.
-
Efficacy of Ertugliflozin on Heart Failure-Related Events in Patients With Type 2 Diabetes Mellitus and Established Atherosclerotic Cardiovascular Disease: Results of the VERTIS CV Trial.Circulation. 2020 Dec 8;142(23):2205-2215. doi: 10.1161/CIRCULATIONAHA.120.050255. Epub 2020 Oct 7. Circulation. 2020. PMID: 33026243 Free PMC article. Clinical Trial.
-
Effects of ertugliflozin on kidney composite outcomes, renal function and albuminuria in patients with type 2 diabetes mellitus: an analysis from the randomised VERTIS CV trial.Diabetologia. 2021 Jun;64(6):1256-1267. doi: 10.1007/s00125-021-05407-5. Epub 2021 Mar 4. Diabetologia. 2021. PMID: 33665685 Free PMC article. Clinical Trial.
-
The Effects of SGLT2 Inhibitors on Cardiovascular and Renal Outcomes in Diabetic Patients: A Systematic Review and Meta-Analysis.Cardiorenal Med. 2020;10(1):1-10. doi: 10.1159/000503919. Epub 2019 Nov 19. Cardiorenal Med. 2020. PMID: 31743918
-
The renoprotective effects of sodium-glucose cotransporter 2 inhibitors versus placebo in patients with type 2 diabetes with or without prevalent kidney disease: A systematic review and meta-analysis.Diabetes Obes Metab. 2019 Apr;21(4):1018-1026. doi: 10.1111/dom.13620. Epub 2019 Jan 16. Diabetes Obes Metab. 2019. PMID: 30565382
Cited by
-
Examining the Impact of Ertugliflozin on Cardiovascular Outcomes in Patients with Diabetes and Metabolic Syndrome: A Systematic Review of Clinical Trials.Pharmaceuticals (Basel). 2024 Jul 11;17(7):929. doi: 10.3390/ph17070929. Pharmaceuticals (Basel). 2024. PMID: 39065779 Free PMC article. Review.
References
-
- Cosentino F., Cannon C.P., Cherney D.Z.I., et al. Efficacy of ertugliflozin on heart failure-related events in patients with type 2 diabetes mellitus and established atherosclerotic cardiovascular disease: results of the VERTIS CV trial. Circulation. 2020;142:2205–2215. doi: 10.1161/CIRCULATIONAHA.120.050255. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
