

Analysis of Hospital Operating Margins and Provision of Safety Net Services
- PMID: 37071422
- PMCID: PMC10114034
- DOI: 10.1001/jamanetworkopen.2023.8785
Analysis of Hospital Operating Margins and Provision of Safety Net Services
Abstract
Importance: Safety net hospitals (SNH) provide many community services. The cost of providing these services is unknown.
Objective: To determine what safety net criteria are associated with differences in hospital operating margin.
Design, setting, and participants: This cross-sectional study of US acute care hospitals from 2017 to 2019 included eligible hospitals identified from US Centers for Medicare & Medicaid Services Cost Reports.
Exposures: Five domains of SNH: undercompensated care measured using the Disproportionate Share Hospital index, uncompensated care, essential community services, neighborhood disadvantage, and sole community hospital and critical access hospital status. Each was categorized as a quintile or binary response. Covariates included hospital ownership, size, teaching status, census region, urbanicity, and wage index.
Main outcomes and measures: Operating margin and its association with each safety net criterion was determined using linear regression adjusting for all safety net criteria and covariates.
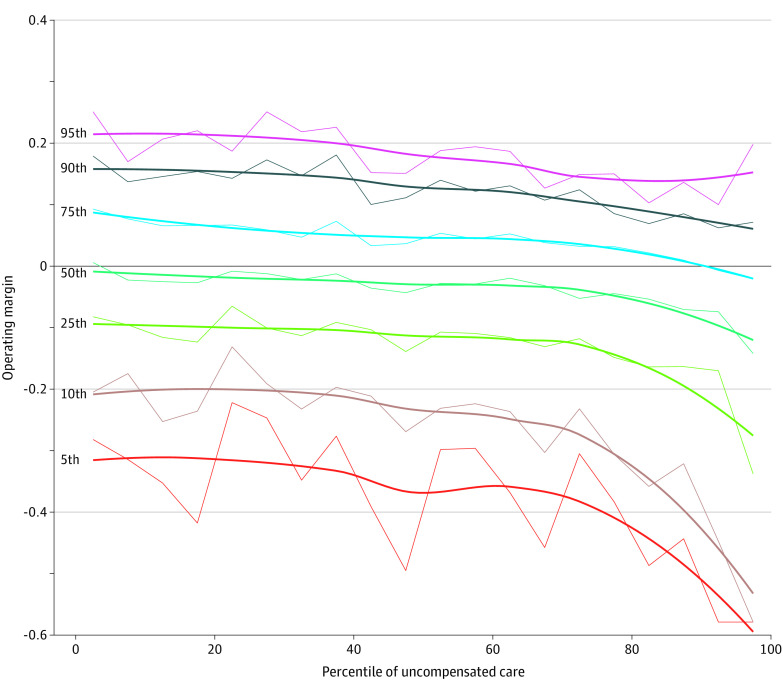
Results: A total of 4219 hospitals were analyzed, of which 3329 hospitals (78.9%) satisfied at least 1 safety net criterion; 23 hospitals (0.5%) met 4 or all 5 criteria. Among safety net criteria, the highest quintile of undercompensated care (-6.2 percentage point difference compared with lowest quintile; 95% CI, -8.2 to -4.2 percentage points), uncompensated care (-3.4 percentage points; 95% CI, -5.1 to -1.6 percentage points), and neighborhood disadvantage (-3.9 percentage points; 95% CI, -5.7 to -2.1 percentage points) were each associated with a lower operating margin. No association with operating margin was found between critical access or sole community hospital status (0.9 percentage points; 95% CI, -0.8 to 2.7 percentage points) or the highest vs lowest quintile of essential services (0.8 percentage points; 95% CI, -1.2 to 2.7 percentage points). Among essential services, burn, inpatient psychiatry, and primary care services were associated with lower operating margin, while others were either not associated or showed positive association. Fall-off in operating margin by level of uncompensated care was most severe in the highest percentiles of uncompensated care, with the most marked declines among those with the lowest operating margin.
Conclusions and relevance: In this cross-sectional study of SNH, hospitals in the highest quintiles of undercompensated care, uncompensated care, and neighborhood disadvantage were more financially vulnerable than those not in the top quintile, especially when they met numerous of these criteria. Ensuring targeting of financial support to these hospitals could improve their financial stability.
Conflict of interest statement
Figures
Similar articles
-
Comparison of 3 Safety-Net Hospital Definitions and Association With Hospital Characteristics.JAMA Netw Open. 2019 Aug 2;2(8):e198577. doi: 10.1001/jamanetworkopen.2019.8577. JAMA Netw Open. 2019. PMID: 31390034 Free PMC article.
-
The Early Impact of the COVID-19 Pandemic on Hospital Finances.J Healthc Manag. 2023 Jan-Feb 01;68(1):38-55. doi: 10.1097/JHM-D-22-00037. J Healthc Manag. 2023. PMID: 36602454
-
Association of Medicaid Expansion With Quality in Safety-Net Hospitals.JAMA Intern Med. 2021 May 1;181(5):590-597. doi: 10.1001/jamainternmed.2020.9142. JAMA Intern Med. 2021. PMID: 33587092 Free PMC article.
-
The supply of uncompensated care in Pennsylvania hospitals: motives and financial consequences.Health Care Manage Rev. 2004 Jul-Sep;29(3):229-39. doi: 10.1097/00004010-200407000-00008. Health Care Manage Rev. 2004. PMID: 15357233 Review.
-
Characteristics of Safety-Net Hospitals, 2014.2016 Oct. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #213. 2016 Oct. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #213. PMID: 27929631 Free Books & Documents. Review.
Cited by
-
Changes in US Hospital Financial Performance During the COVID-19 Public Health Emergency.JAMA Health Forum. 2023 Jul 7;4(7):e231928. doi: 10.1001/jamahealthforum.2023.1928. JAMA Health Forum. 2023. PMID: 37450295 Free PMC article.
-
Strengthening essential emergency departments: Transforming the safety net.Health Aff Sch. 2025 Mar 3;3(3):qxaf044. doi: 10.1093/haschl/qxaf044. eCollection 2025 Mar. Health Aff Sch. 2025. PMID: 40084221 Free PMC article.
-
Associations of U.S. hospital closure (2007-2018) with area socioeconomic disadvantage and racial/ethnic composition.Ann Epidemiol. 2024 Apr;92:40-46. doi: 10.1016/j.annepidem.2024.02.010. Epub 2024 Mar 2. Ann Epidemiol. 2024. PMID: 38432535 Free PMC article.
-
Structural Discrimination in Nonprofit Hospital Community Benefit Spending.JAMA Health Forum. 2025 Feb 7;6(2):e245523. doi: 10.1001/jamahealthforum.2024.5523. JAMA Health Forum. 2025. PMID: 40019742 Free PMC article.
-
Barriers and Facilitators to Establishing Partnerships for Substance Use Disorder Care Transitions Between Safety-Net Hospitals and Community-Based Organizations.J Gen Intern Med. 2024 Sep;39(12):2150-2159. doi: 10.1007/s11606-024-08883-8. Epub 2024 Jun 27. J Gen Intern Med. 2024. PMID: 38937366
References
-
- Sutton JP, Washington RE, Fingar KR, Elixhauser A. Statistical Brief #213: Characteristics of Safety-Net Hospitals, 2014. Healthcare Cost & Utilization Project. October 2016. Accessed January 20, 2021. https://hcup-us.ahrq.gov/reports/statbriefs/sb213-Safety-Net-Hospitals-2...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
