

A retrospective study on epidemiological analysis of pre-hospital emergency care in Hangzhou, China
- PMID: 37071636
- PMCID: PMC10112809
- DOI: 10.1371/journal.pone.0282870
A retrospective study on epidemiological analysis of pre-hospital emergency care in Hangzhou, China
Abstract
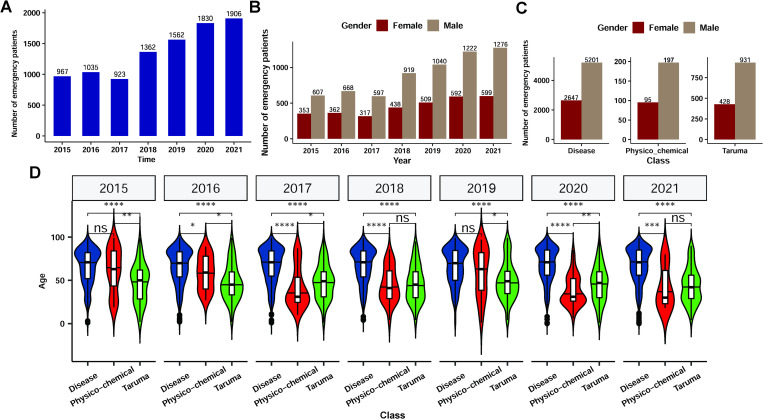
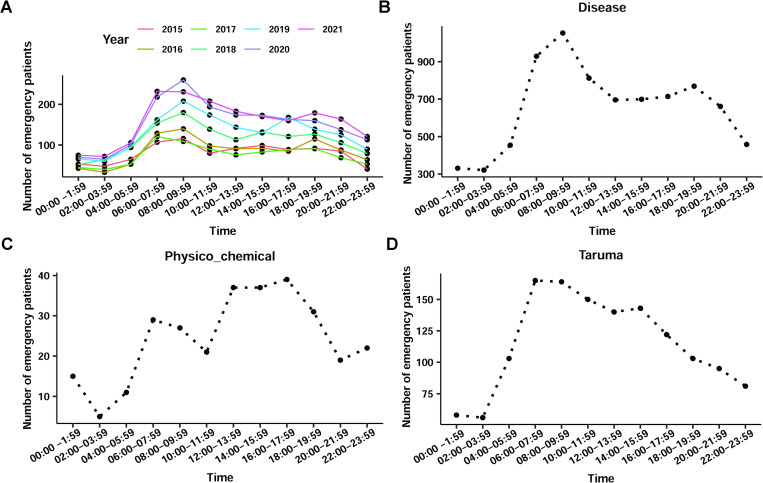
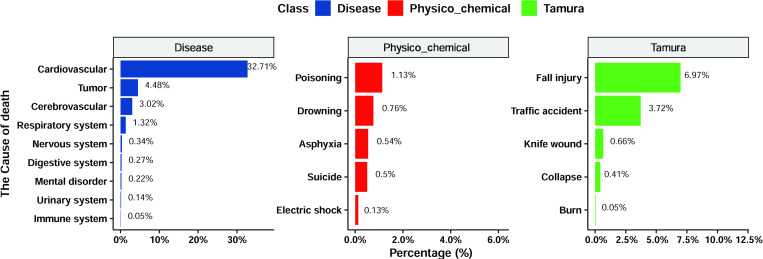
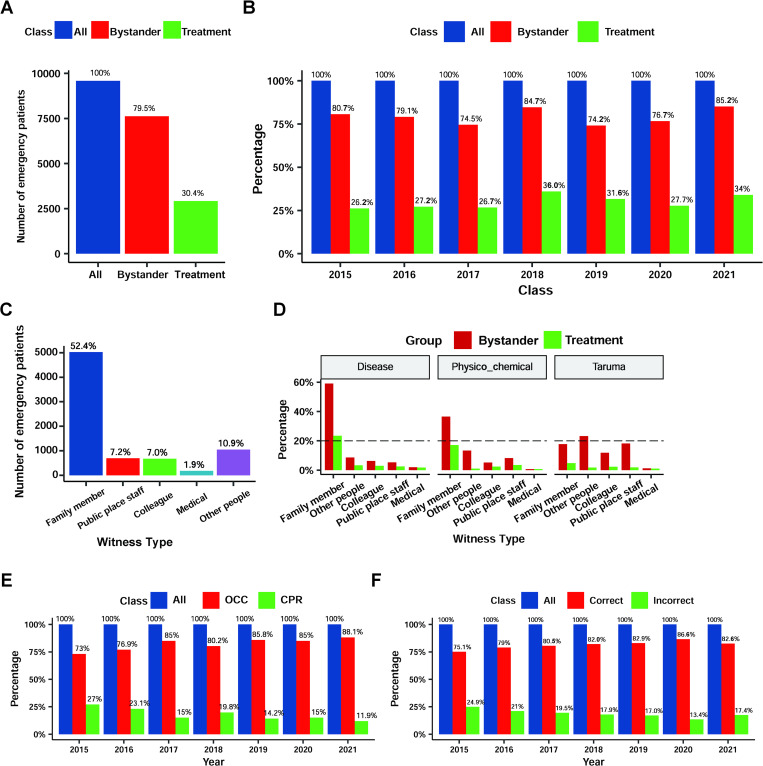
Out-of-hospital cardiac arrest (OHCA) is a leading cause of global mortality, with numerous factors influencing the patient survival rate and prognosis. This study aimed to evaluate the OHCA epidemiology in China and elaborate on the current Hangzhou emergency system status. This retrospective analysis was based on the medical history system of the Hangzhou Emergency Center registered from 2015-2021. We provided a detailed description of OHCA characteristics and investigated the factors affecting the success rate of emergency treatment in terms of epidemiology, causes of onset, bystander rescue, and outcome factors. We included 9585 out-of-hospital cardiac arrest cases, of which 5442 (56.8%) had evidence of resuscitation. Patients with underlying diseases constituted the vast majority (80.1%); trauma and physicochemical factors accounted for 16.5% and 3.4%, respectively. Only 30.4% of patients (about 80.0% of bystanders witnessed) received bystander first aid. The outcome rate of emergency doctors dispatched by emergency centres was significantly higher than doctors dispatched by hospitals. Additionally, physician's first-aid experience, emergency response time, emergency telephone availability, initial heart rhythm, out-of-hospital defibrillation, out-of-hospital intubation, and using of epinephrine significantly can significantly improve the out-of-hospital return of spontaneous circulation in patients. All steps in pre-hospital care are important for patients, especially for bystander first aid and physician's first-aid experience. The popularity of first-aid training and the public emergency medical system are not potent enough. We should take those key factors into consideration when developing a pre-hospital care system for OHCA.
Copyright: © 2023 Wang et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
[Investigation of out-of-hospital cardiac arrest in Zhengzhou City and the risk factors of prognosis of cardiopulmonary resuscitation: case analysis for 2016-2018].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Apr;31(4):439-443. doi: 10.3760/cma.j.issn.2095-4352.2019.04.013. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 31109417 Chinese.
-
Out-of-hospital cardiac arrest surveillance --- Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005--December 31, 2010.MMWR Surveill Summ. 2011 Jul 29;60(8):1-19. MMWR Surveill Summ. 2011. PMID: 21796098
-
[Current status analysis of bystander cardiopulmonary resuscitation for out-of-hospital cardiac arrest in Qinhuangdao region based on Utstein model].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Sep;32(9):1096-1100. doi: 10.3760/cma.j.cn121430-20200714-00520. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 33081897 Chinese.
-
Community first responders for out-of-hospital cardiac arrest in adults and children.Cochrane Database Syst Rev. 2019 Jul 19;7(7):CD012764. doi: 10.1002/14651858.CD012764.pub2. Cochrane Database Syst Rev. 2019. PMID: 31323120 Free PMC article.
-
The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis.Crit Care. 2020 Feb 22;24(1):61. doi: 10.1186/s13054-020-2773-2. Crit Care. 2020. PMID: 32087741 Free PMC article.
Cited by
-
Analysis of the effects of MIPPO under the anterolateral approach on stress indicators and ankle joint function in patients with open fracture of tibia and fibula.BMC Surg. 2025 Jul 3;25(1):273. doi: 10.1186/s12893-025-03030-4. BMC Surg. 2025. PMID: 40611190 Free PMC article.
-
Comprehensive analysis of vulnerability status and associated affect factors among prehospital emergency patients: a single-center descriptive cross-sectional study.Front Public Health. 2024 Feb 29;12:1330194. doi: 10.3389/fpubh.2024.1330194. eCollection 2024. Front Public Health. 2024. PMID: 38487181 Free PMC article.
-
Incidence and temporal trends of out-of-hospital cardiac arrest in Shenzhen, China (2011-2018).Resusc Plus. 2025 Jan 28;22:100882. doi: 10.1016/j.resplu.2025.100882. eCollection 2025 Mar. Resusc Plus. 2025. PMID: 40008323 Free PMC article.
-
Sudden cardiac arrest mortality in China: temporal trends and risk factors.Mil Med Res. 2025 Aug 15;12(1):49. doi: 10.1186/s40779-025-00639-7. Mil Med Res. 2025. PMID: 40813723 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
