

Bladder cancer organoids as a functional system to model different disease stages and therapy response
- PMID: 37072390
- PMCID: PMC10113240
- DOI: 10.1038/s41467-023-37696-2
Bladder cancer organoids as a functional system to model different disease stages and therapy response
Abstract
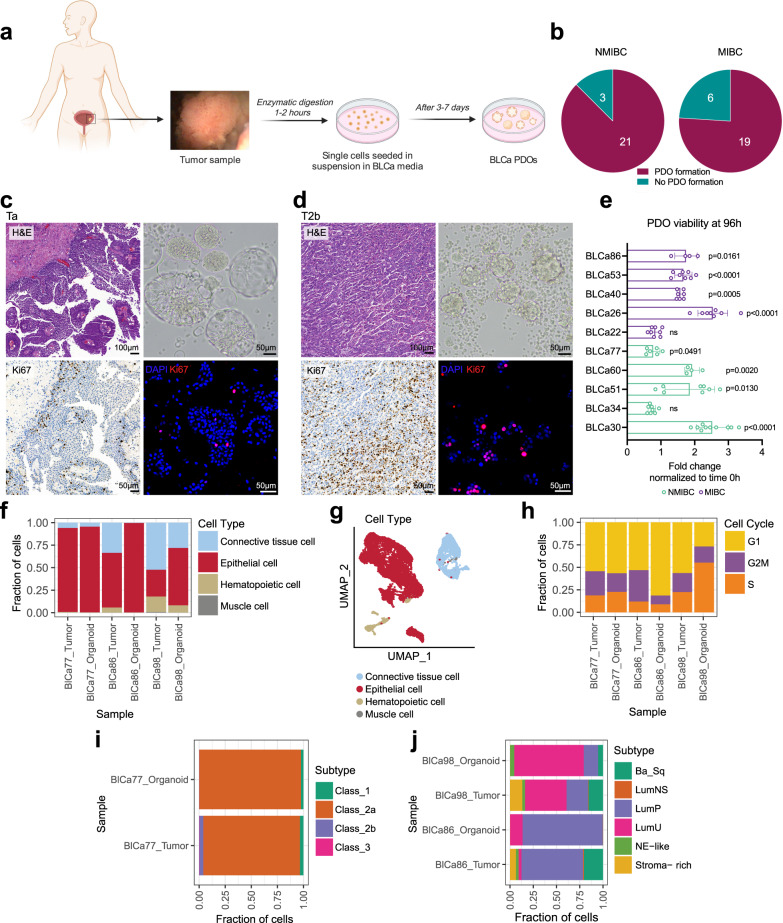
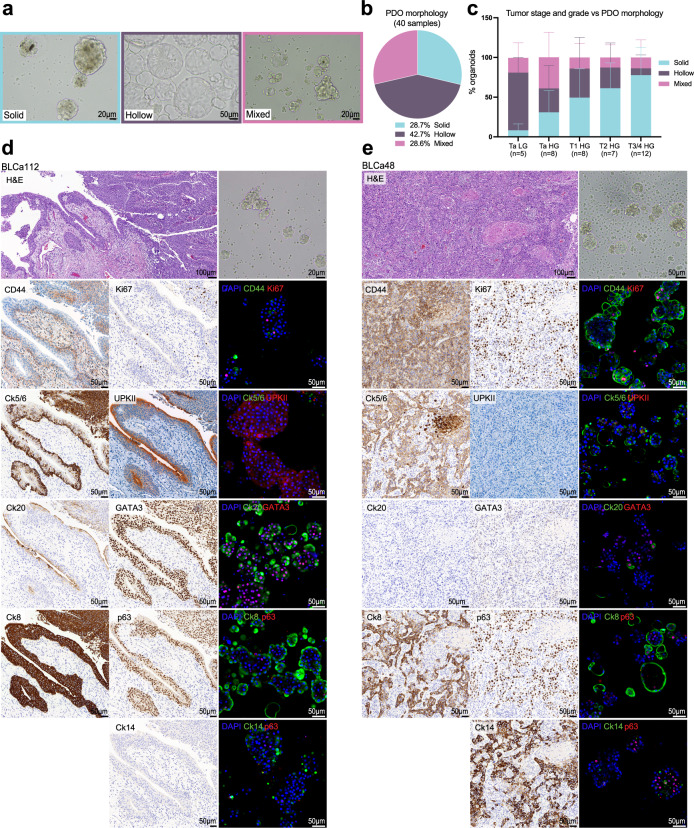
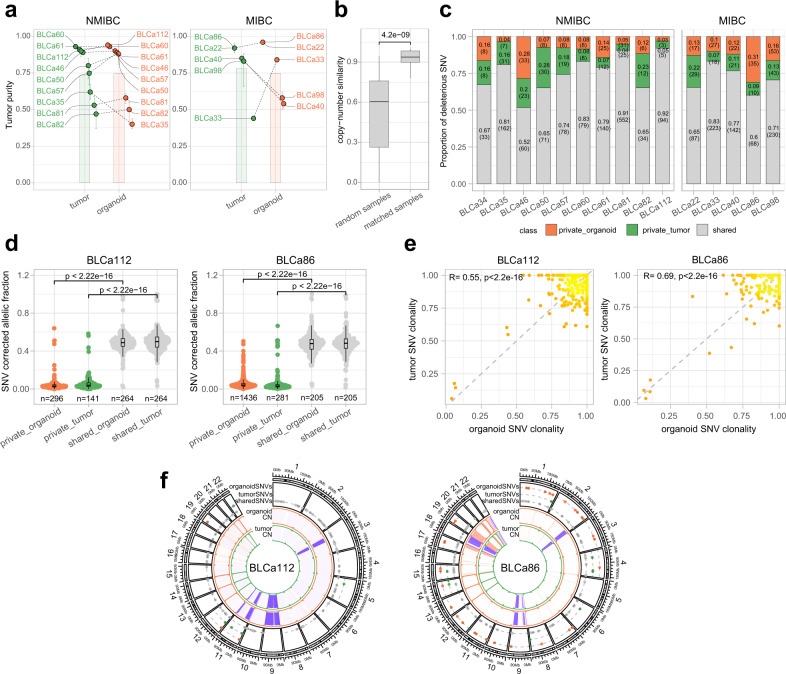
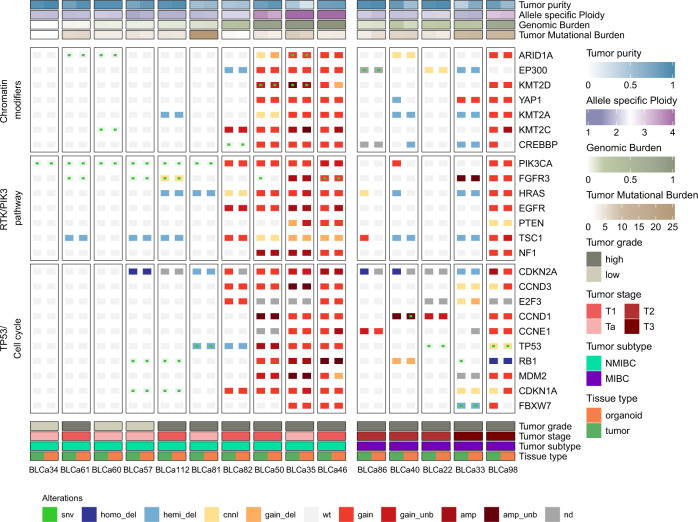
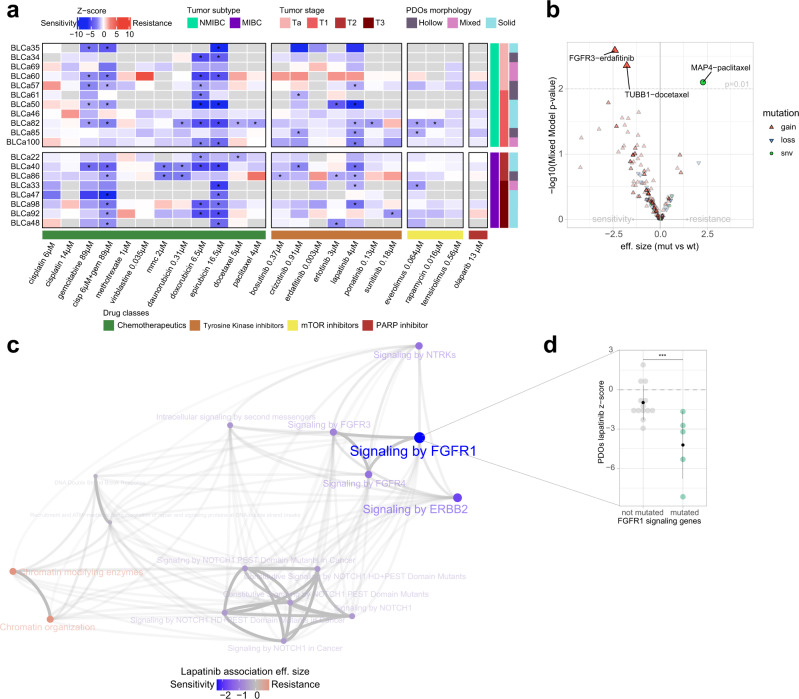
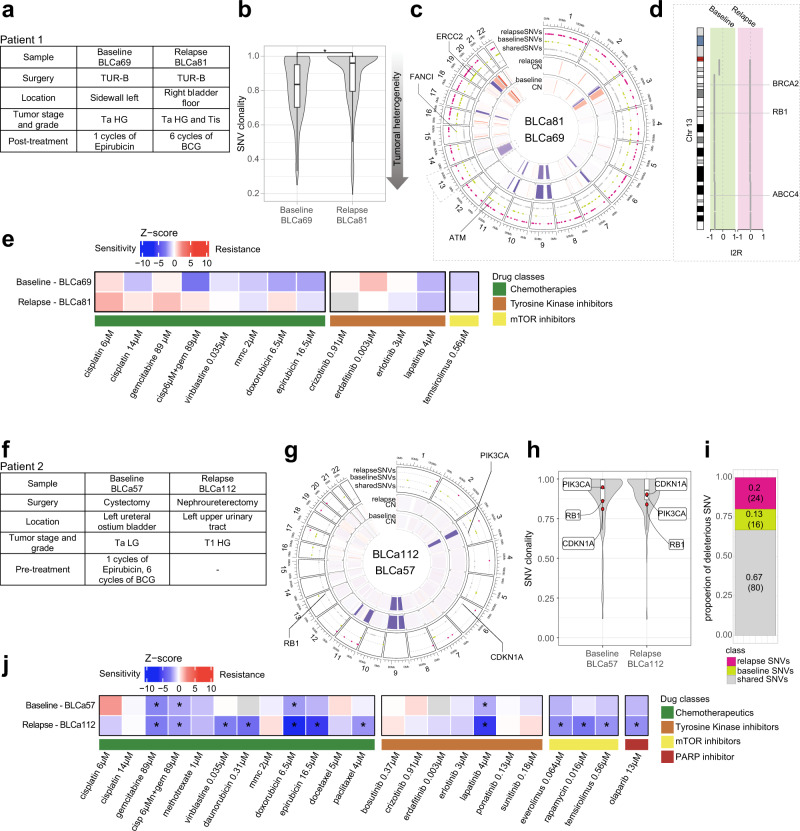
Bladder Cancer (BLCa) inter-patient heterogeneity is the primary cause of treatment failure, suggesting that patients could benefit from a more personalized treatment approach. Patient-derived organoids (PDOs) have been successfully used as a functional model for predicting drug response in different cancers. In our study, we establish PDO cultures from different BLCa stages and grades. PDOs preserve the histological and molecular heterogeneity of the parental tumors, including their multiclonal genetic landscapes, and consistently share key genetic alterations, mirroring tumor evolution in longitudinal sampling. Our drug screening pipeline is implemented using PDOs, testing standard-of-care and FDA-approved compounds for other tumors. Integrative analysis of drug response profiles with matched PDO genomic analysis is used to determine enrichment thresholds for candidate markers of therapy response and resistance. Finally, by assessing the clinical history of longitudinally sampled cases, we can determine whether the disease clonal evolution matched with drug response.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Uro-Science.J Urol. 2023 Dec;210(6):922-924. doi: 10.1097/JU.0000000000003662. Epub 2023 Sep 29. J Urol. 2023. PMID: 37774378 No abstract available.
Similar articles
-
Patient-derived Organoids in Bladder Cancer: Opportunities and Challenges.Eur Urol Focus. 2025 Jan;11(1):62-70. doi: 10.1016/j.euf.2024.08.008. Epub 2024 Sep 3. Eur Urol Focus. 2025. PMID: 39232905 Review.
-
Patient-Derived Bladder Cancer Organoids as a Valuable Tool for Understanding Tumor Biology and Developing Personalized Treatment.Adv Sci (Weinh). 2025 Apr;12(13):e2414558. doi: 10.1002/advs.202414558. Epub 2025 Feb 7. Adv Sci (Weinh). 2025. PMID: 39921252 Free PMC article.
-
Modeling bladder cancer in the laboratory: Insights from patient-derived organoids.Biochim Biophys Acta Rev Cancer. 2024 Nov;1879(6):189199. doi: 10.1016/j.bbcan.2024.189199. Epub 2024 Oct 15. Biochim Biophys Acta Rev Cancer. 2024. PMID: 39419296 Review.
-
Patient-derived organoid culture of gastric cancer for disease modeling and drug sensitivity testing.Biomed Pharmacother. 2023 Jul;163:114751. doi: 10.1016/j.biopha.2023.114751. Epub 2023 Apr 26. Biomed Pharmacother. 2023. PMID: 37105073
-
Genomic characteristics and drug screening among organoids derived from non-small cell lung cancer patients.Thorac Cancer. 2020 Aug;11(8):2279-2290. doi: 10.1111/1759-7714.13542. Epub 2020 Jul 7. Thorac Cancer. 2020. PMID: 32633046 Free PMC article.
Cited by
-
Prospective pharmacotyping of urothelial carcinoma organoids for drug sensitivity prediction - feasibility and real world experience.Exp Hematol Oncol. 2024 Nov 12;13(1):112. doi: 10.1186/s40164-024-00579-3. Exp Hematol Oncol. 2024. PMID: 39533373 Free PMC article.
-
Patient-derived tumor organoids: A preclinical platform for personalized cancer therapy.Transl Oncol. 2025 Jan;51:102226. doi: 10.1016/j.tranon.2024.102226. Epub 2024 Dec 1. Transl Oncol. 2025. PMID: 39622151 Free PMC article. Review.
-
Human organoids-on-chips for biomedical research and applications.Theranostics. 2024 Jan 1;14(2):788-818. doi: 10.7150/thno.90492. eCollection 2024. Theranostics. 2024. PMID: 38169573 Free PMC article. Review.
-
The role of organoids in cancer research.Exp Hematol Oncol. 2023 Aug 3;12(1):69. doi: 10.1186/s40164-023-00433-y. Exp Hematol Oncol. 2023. PMID: 37537666 Free PMC article. Review.
-
Multi-omics analysis unveils the predictive value of IGF2BP3/SPHK1 signaling in cancer stem cells for prognosis and immunotherapeutic response in muscle-invasive bladder cancer.J Transl Med. 2024 Oct 4;22(1):900. doi: 10.1186/s12967-024-05685-8. J Transl Med. 2024. PMID: 39367493 Free PMC article.
References
-
- Soukup V, et al. Prognostic performance and reproducibility of the 1973 and 2004/2016 World Health Organization grading classification systems in non-muscle-invasive bladder cancer: a European Association of Urology Non-muscle Invasive Bladder Cancer Guidelines Panel systematic review. Eur. Urol. 2017;72:801–813. doi: 10.1016/j.eururo.2017.04.015. - DOI - PubMed
-
- Miller KD, et al. Cancer treatment and survivorship statistics, 2016. CA: A Cancer J. Clin. 2016;66:271–289. - PubMed
-
- Facchini G, et al. Advanced/metastatic bladder cancer: current status and future directions. Eur. Rev. Med. Pharm. Sci. 2020;24:11536–11552. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
