

Use of the Spirometric "Fixed-Ratio" Underdiagnoses COPD in African-Americans in a Longitudinal Cohort Study
- PMID: 37072532
- PMCID: PMC10593702
- DOI: 10.1007/s11606-023-08185-5
Use of the Spirometric "Fixed-Ratio" Underdiagnoses COPD in African-Americans in a Longitudinal Cohort Study
Abstract
Background: COPD diagnosis is tightly linked to the fixed-ratio spirometry criteria of FEV1/FVC < 0.7. African-Americans are less often diagnosed with COPD.
Objective: Compare COPD diagnosis by fixed-ratio with findings and outcomes by race.
Design: Genetic Epidemiology of COPD (COPDGene) (2007-present), cross-sectional comparing non-Hispanic white (NHW) and African-American (AA) participants for COPD diagnosis, manifestations, and outcomes.
Setting: Multicenter, longitudinal US cohort study.
Participants: Current or former smokers with ≥ 10-pack-year smoking history enrolled at 21 clinical centers including over-sampling of participants with known COPD and AA. Exclusions were pre-existing non-COPD lung disease, except for a history of asthma.
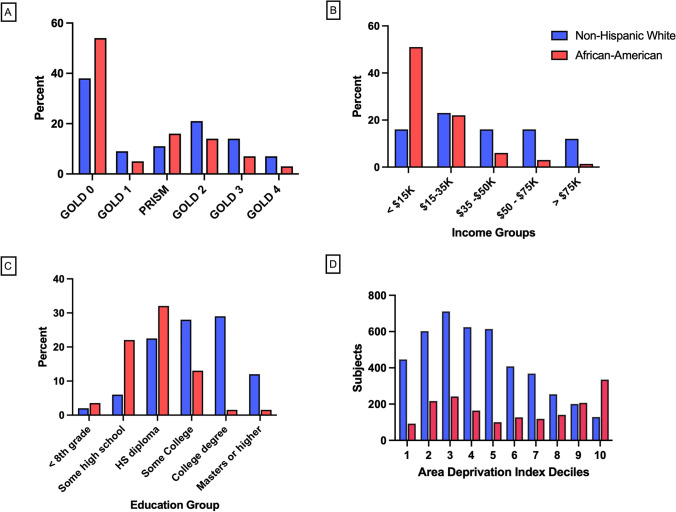
Measurements: Subject diagnosis by conventional criteria. Mortality, imaging, respiratory symptoms, function, and socioeconomic characteristics, including area deprivation index (ADI). Matched analysis (age, sex, and smoking status) of AA vs. NHW within participants without diagnosed COPD (GOLD 0; FEV1 ≥ 80% predicted and FEV1/FVC ≥ 0.7).
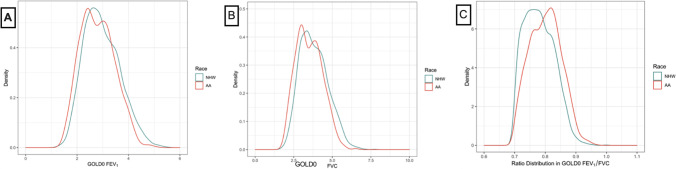
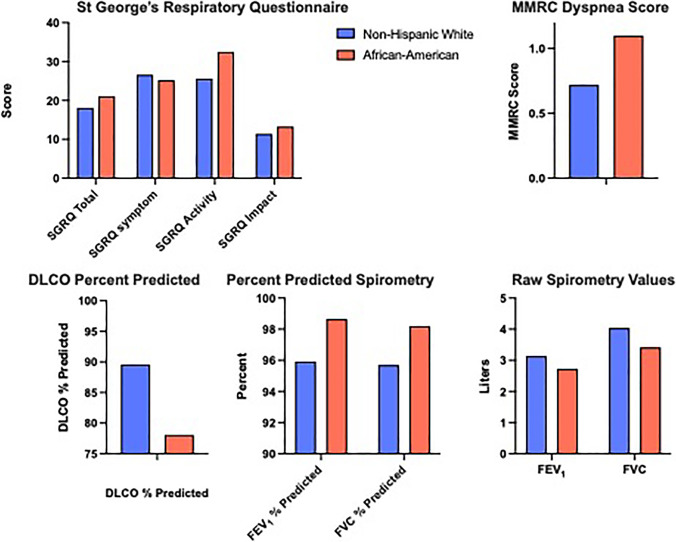
Results: Using the fixed ratio, 70% of AA (n = 3366) were classified as non-COPD, versus 49% of NHW (n = 6766). AA smokers were younger (55 vs. 62 years), more often current smoking (80% vs. 39%), with fewer pack-years but similar 12-year mortality. Density distribution plots for FEV1 and FVC raw spirometry values showed disproportionate reductions in FVC relative to FEV1 in AA that systematically led to higher ratios. The matched analysis demonstrated GOLD 0 AA had greater symptoms, worse DLCO, spirometry, BODE scores (1.03 vs 0.54, p < 0.0001), and greater deprivation than NHW.
Limitations: Lack of an alternative diagnostic metric for comparison.
Conclusions: The fixed-ratio spirometric criteria for COPD underdiagnosed potential COPD in AA participants when compared to broader diagnostic criteria. Disproportionate reductions in FVC relative to FEV1 leading to higher FEV1/FVC were identified in these participants and associated with deprivation. Broader diagnostic criteria for COPD are needed to identify the disease across all populations.
Keywords: COPD; deprivation; diagnosis; fixed ratio; spirometry.
© 2023. The Author(s), under exclusive licence to Society of General Internal Medicine.
Conflict of interest statement
The project described was supported by Award Number U01 HL089897 and Award Number U01 HL089856 from the National Heart, Lung, and Blood Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute or the National Institutes of Health.
Figures
References
-
- Committee GS. Global Initiative for Chronic Obstructive Lung Disease 2023 Report. 2023.
-
- Committee GS. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2021 Global Initiative for Chronic Obstructive Lung Disease, Inc; 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
