

Extracorporeal cardiopulmonary resuscitation dissemination and integration with organ preservation in the USA: ethical and logistical considerations
- PMID: 37072806
- PMCID: PMC10111746
- DOI: 10.1186/s13054-023-04432-7
Extracorporeal cardiopulmonary resuscitation dissemination and integration with organ preservation in the USA: ethical and logistical considerations
Abstract
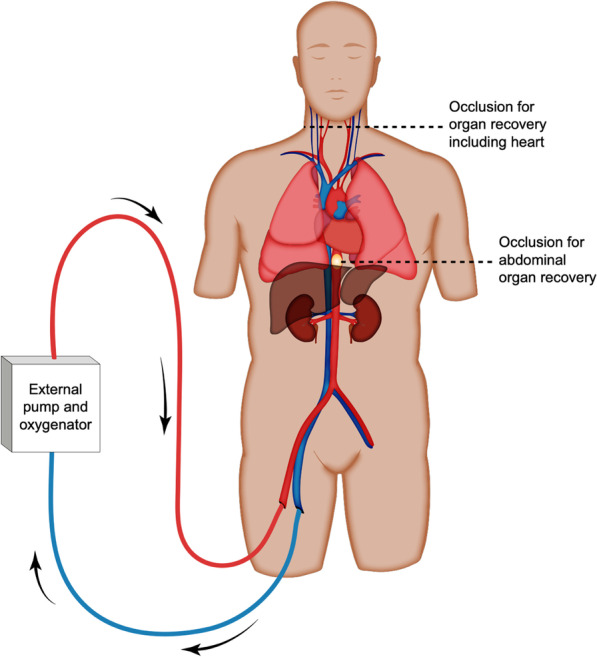
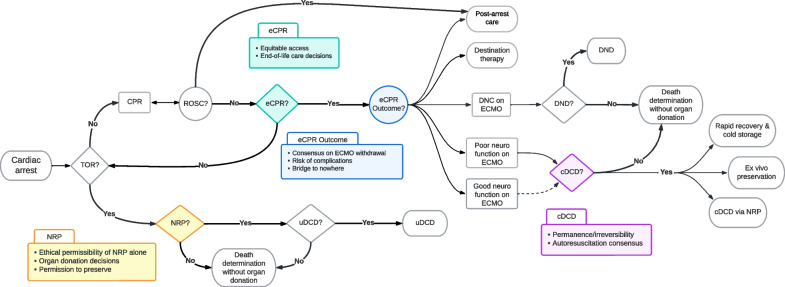
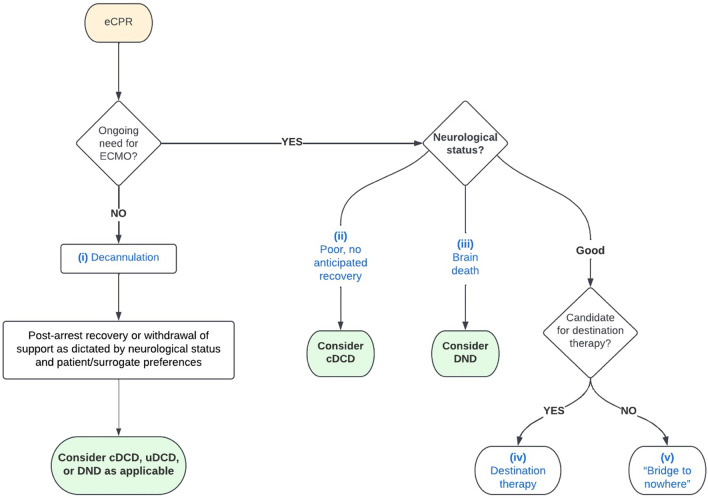
Use of extracorporeal membrane oxygenation (ECMO) in cardiopulmonary resuscitation, termed eCPR, offers the prospect of improving survival with good neurological function after cardiac arrest. After death, ECMO can also be used for enhanced preservation of abdominal and thoracic organs, designated normothermic regional perfusion (NRP), before organ recovery for transplantation. To optimize resuscitation and transplantation outcomes, healthcare networks in Portugal and Italy have developed cardiac arrest protocols that integrate use of eCPR with NRP. Similar dissemination of eCPR and its integration with NRP in the USA raise novel ethical issues due to a non-nationalized health system and an opt-in framework for organ donation, as well as other legal and cultural factors. Nonetheless, eCPR investigations are ongoing, and both eCPR and NRP are selectively employed in clinical practice. This paper delineates the most pressing relevant ethical considerations and proposes recommendations for implementation of protocols that aim to promote public trust and reduce conflicts of interest. Transparent policies should rely on protocols that separate lifesaving from organ preservation considerations; robust, centralized eCPR data to inform equitable and evidence-based allocations; uniform practices concerning clinical decision-making and resource utilization; and partnership with community stakeholders, allowing patients to make decisions about emergency care that align with their values. Proactively addressing these ethical and logistical challenges could enable eCPR dissemination and integration with NRP protocols in the USA, with the potential to maximize lives saved through both improved resuscitation with good neurological outcomes and increased organ donation opportunities when resuscitation is unsuccessful or not in accordance with individuals' wishes.
Keywords: Bioethics; Cardiopulmonary resuscitation; Extracorporeal membrane oxygenation; Organ donation; Organ preservation.
© 2023. The Author(s).
Conflict of interest statement
Disclosure for Robert Montgomery: Advisory Boards: eGenesis, Sanofi, Regeneron, CareDx, Hansa Biopharma. Strategic consultant: Recombinetics. Consulting fees and/or travel expenses: Hansa Medical, Regeneron, ThermoFisher Scientific Genentech, CareDx, One Lambda, ITB Med, Sanofi & PPD Development. Research Grants: Lung Biotechnologies (United Therapeutics) & Hansa Biopharma. Disclosure for Brendan Parent: Director of program supported by a gift from United Therapeutics. Disclosure for Tamar Schiff: Salary supported by a gift from United Therapeutics.
Figures
References
-
- Hessheimer AJ, Fondevila C. Normothermic regional perfusion in solid organ transplantation. advances in extracorporeal membrane oxygenation-Volume 3: IntechOpen; 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
