

Safety and effectiveness of standardized exercise training in patients with pulmonary hypertension associated with heart failure with preserved ejection fraction (TRAIN-HFpEF-PH): study protocol for a randomized controlled multicenter trial
- PMID: 37072812
- PMCID: PMC10114476
- DOI: 10.1186/s13063-023-07297-x
Safety and effectiveness of standardized exercise training in patients with pulmonary hypertension associated with heart failure with preserved ejection fraction (TRAIN-HFpEF-PH): study protocol for a randomized controlled multicenter trial
Abstract
Background: Left heart failure (HF) is characterized by an elevation in left-sided filling pressures, causing symptoms of dyspnea, impairing exercise capacity, and leading to pulmonary venous congestion and secondary pulmonary hypertension (PH). There is an increased incidence of PH associated with left heart disease, particularly with heart failure with preserved ejection fraction (HFpEF-PH). Treatment possibilities in HFpEF-PH are non-specific and very limited, thus additional pharmacological and non-pharmacological therapeutic strategies are needed. Various types of exercise-based rehabilitation programs have been shown to improve exercise capacity and quality of life (QoL) of HF and PH patients. However, no study focused on exercise training in the population of HFpEF-PH. This study is designed to investigate whether a standardized low-intensity exercise and respiratory training program is safe and may improve exercise capacity, QoL, hemodynamics, diastolic function, and biomarkers in patients with HFpEF-PH.
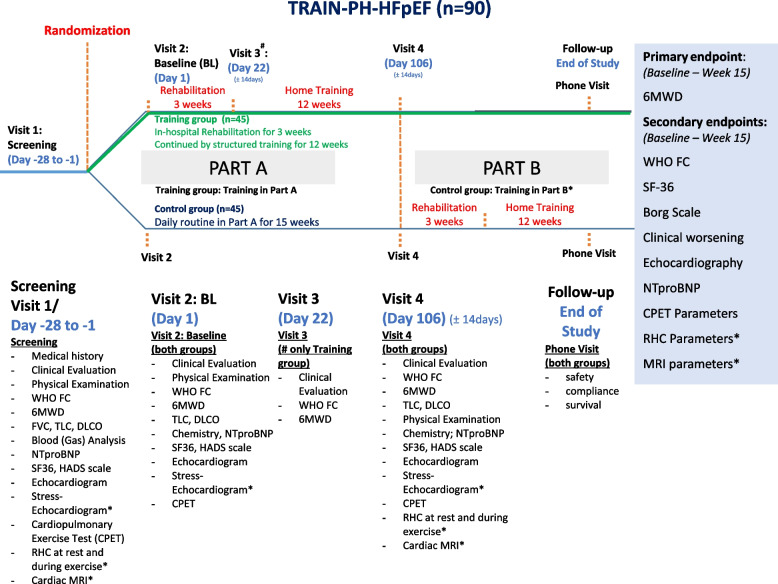
Methods: A total of 90 stable patients with HFpEF-PH (World Health Organization functional class II-IV) will be randomized (1:1) to receive a 15-week specialized low-intensity rehabilitation program, including exercise and respiratory therapy and mental gait training, with an in-hospital start, or standard care alone. The primary endpoint of the study is a change in 6-min walk test distance; secondary endpoints are changes in peak exercise oxygen uptake, QoL, echocardiographic parameters, prognostic biomarkers, and safety parameters.
Discussion: To date, no study has investigated the safety and efficacy of exercising specifically in the HFpEF-PH population. We believe that a randomized controlled multicenter trial, which protocol we are sharing in this article, will add important knowledge about the potential utility of a specialized low-intensity exercise and respiratory training program for HFpEF-PH and will be valuable in finding optimal treatment strategies for these patients.
Trial registration: ClinicalTrials.gov NCT05464238. July 19, 2022.
Keywords: Exercise training; Heart failure with preserved ejection fraction; Pulmonary hypertension; Randomized controlled trial; Study protocol.
© 2023. The Author(s).
Conflict of interest statement
E.P. reports speaker honoraria fees from Johnson and Johnson and Medis Pharma outside this work.
J.Č. reports personal fees from AstraZeneca, Boehringer Ingelheim, Pfizer, Bayer, and Novartis outside this work.
E.G. reports research grants and speaker honoraria/consultancy fees from Actelion, Janssen, Bayer, MSD, Merck, and Ferrer and research grants to the institution from Acceleron, Actelion, Bayer, MSD, Janssen, Liquidia, United Therapeutics, and OMT outside the submitted work.
L.G. has received speaker’s fees from Actelion, Johnson & Johnson, and Medis Pharma outside the submitted work.
S.Č. reports honoraria fees from Medtronic, Bostopn Scientific, and Meril outside this work.
T.Š., C.A.E, N.B., E.J., and D.Z. declare that they have no competing interests.
Similar articles
-
Inspiratory Muscle Training and Functional Electrical Stimulation for Treatment of Heart Failure With Preserved Ejection Fraction: Rationale and Study Design of a Prospective Randomized Controlled Trial.Clin Cardiol. 2016 Aug;39(8):433-9. doi: 10.1002/clc.22555. Epub 2016 Aug 2. Clin Cardiol. 2016. PMID: 27481035 Free PMC article. Clinical Trial.
-
Effects of inspiratory muscle training in patients with heart failure with preserved ejection fraction.Eur J Prev Cardiol. 2014 Dec;21(12):1465-73. doi: 10.1177/2047487313498832. Epub 2013 Jul 17. Eur J Prev Cardiol. 2014. PMID: 23864363 Clinical Trial.
-
Effect of exercise training in patients with chronotropic incompetence and heart failure with preserved ejection fraction: Training-HR study protocol.Curr Probl Cardiol. 2024 Dec;49(12):102839. doi: 10.1016/j.cpcardiol.2024.102839. Epub 2024 Sep 4. Curr Probl Cardiol. 2024. PMID: 39242065
-
Impact of exercise training on exercise tolerance, cardiac function and quality of life in individuals with heart failure and preserved ejection fraction: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2025 Mar 25;25(1):217. doi: 10.1186/s12872-025-04649-0. BMC Cardiovasc Disord. 2025. PMID: 40133870 Free PMC article.
-
Exercise training in Diastolic Heart Failure (Ex-DHF): rationale and design of a multicentre, prospective, randomized, controlled, parallel group trial.Eur J Heart Fail. 2017 Aug;19(8):1067-1074. doi: 10.1002/ejhf.862. Epub 2017 May 17. Eur J Heart Fail. 2017. PMID: 28516519 Review.
Cited by
-
Association of daily physical activity with pulmonary artery pressure in HFpEF and HFmrEF NYHA class III patients: a pilot trial-feasibility and first results.Clin Res Cardiol. 2024 Nov 7. doi: 10.1007/s00392-024-02564-6. Online ahead of print. Clin Res Cardiol. 2024. PMID: 39508889
References
-
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, Carlsen J, Coats AJS, Escribano-Subias P, Ferrari P, Ferreira DS, Ghofrani HA, Giannakoulas G, Kiely DG, Mayer E, Meszaros G, Nagavci B, Olsson KM, Pepke-Zaba J, Quint JK, Rådegran G, Simonneau G, Sitbon O, Tonia T, Toshner M, Vachiery JL, Vonk Noordegraaf A, Delcroix M, Rosenkranz S; ESC/ERS Scientific Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2023;61(1):2200879. 10.1183/13993003.00879-2022. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
